|
|
Hypertrophic Osteoarthropathy
Hypertrophic Pulmonary Osteoarthropathy
General Considerations
- Clinical syndrome consisting of clubbing of the fingers and toes
- Painful and swollen joints
- Symmetric periostitis especially involving the tibia and fibula, radius and ulna
- Most often secondary to an intrathoracic neoplasm or infection
- Primary form is called pachydermoperiostitis
Etiology
- Release of vasodilators which are not metabolized by lung
- Increased flow through AV shunts
- Reflex peripheral vasodilation (vagal impulses)
- Hormones: estrogen, growth hormone, prostaglandin
Thoracic Causes
- Malignant tumor (0.7-12%)
- Benign tumor
- Chronic infection / inflammation
- Congenital heart disease with R-to-L shunt
Extrathoracic Causes
- GI tract
- Liver disease
- Biliary + alcoholic cirrhosis
- Posthepatic cirrhosis
- Chronic active hepatitis
- Bile duct carcinoma
- Benign bile duct stricture
- Amyloidosis, liver
- Abscess
- Undifferentiated nasopharyngeal carcinoma
- Pancreatic carcinoma
- Chronic myelogenous leukemia
Clinical Findings
- Burning pain
- Painful swelling of limbs
- Stiffness of joints
- Ankles (88%)
- Wrists (83%)
- Knees (75%)
- Elbows (17%)
- Shoulders (10%)
- Fingers (7%)
- Peripheral neurovascular disorders
- Local cyanosis
- Areas of increased sweating
- Parasthesia
- Chronic erythema
- Flushing and blanching of skin
- Clubbing
- Hypertrophy of extremities (soft-tissue swelling)
Location
- Tibia and fibula (75%)
- Radius and ulna (80%)
- Proximal phalanges (60%), femur (50%)
- Metacarpus and metatarsus (40%), humerus and distal phalanges (25%)
- Pelvis (5%)
- Unilateral (rare)
Imaging Findings
- In diametaphyseal regions
- Periosteal proliferation of new bone
- First smooth, then undulating rough, most conspicuous on concavity of long bones (dorsal and medial aspects)
- Regression of periosteal reaction after thoracotomy
- Soft-tissue swelling ("clubbing") of distal phalanges
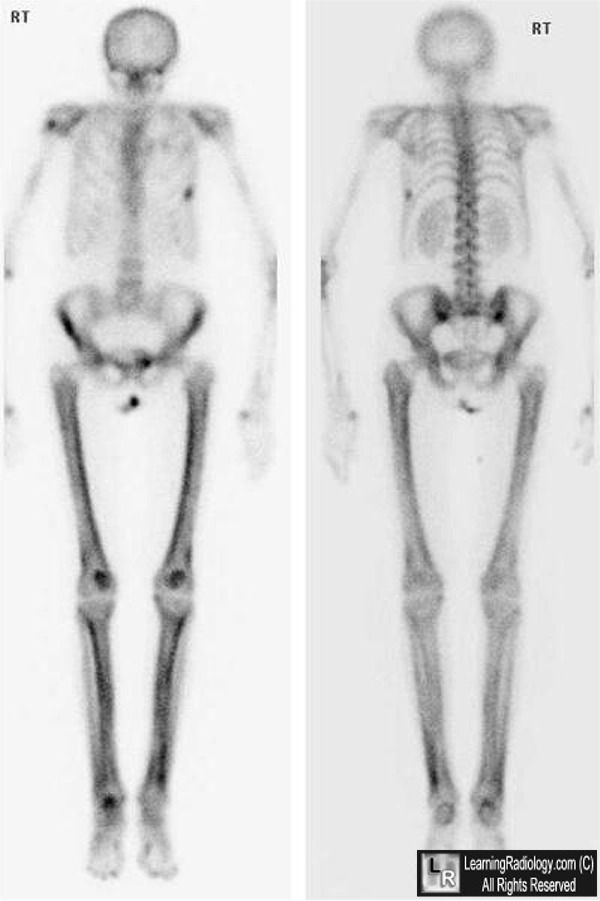
- Bone scan reveals changes early with greater sensitivity and clarity
- Symmetric diffusely increased uptake along cortical margins of diaphysis and metaphysis of tubular bones of the extremities
- Increased periarticular uptake (synovitis)
- Scapular involvement in 2/3
- Mandible ± maxilla abnormal in 40%
 
Hypertrophic Osteoarthropathy. Bone scan (above left) shows symmetric, bilateral,
linear uptake in the femurs and tibias (black arrows) while the conventional radiographs
of the distal femurs and proximal tibias (above right) show smooth, wavy periosteal reaction
primarily involving the metadiaphyseal portion of the bones (white arrows).
For these same photos without the arrows, click here and here

Hypertrophic Osteoarthropathy. Frontal and lateral radiograph of the distal femur
shows a thick, wavy periosteal reaction that involves the diaphysis but spares the epiphysis
For more information, click on the link if you see this icon 
|
|
|

{kind=link}
{kind=link}