|
Bronchiectasis
•
Pathologic dilation of the medium sized airways
•
Proximal bronchiectasis is characteristic of allergic bronchopulmonary
aspergillosis (ABPA)
•
Classical clinical triad: chronic cough, excess sputum production and repeated
infection
Pathogenesis
• Three major causes are: obstruction, infection and traction
• Bronchiectasis is common when there is prolonged partial
obstruction, e.g. slow-growing neoplasms, foreign bodies
• Infection is most important cause of bronchiectasis
• Bronchial wall destruction occurs in infection
• Traction comes from a force, usually due to increased elastic
recoil in the surrounding lung, which pulls the bronchus and dilates it
Location
• Bronchiectasis from viral or pyogenic infections is usually at the
bases
• Tuberculous bronchiectasis is usually at the apices
• Diffuse bronchiectasis
§ Impaired mucus clearing e.g. cystic fibrosis and Kartagener Syndrome
§ ABPA
§ Chronic diffuse airways disease (chronic bronchitis, asthma, bronchiolitis obliterans
§ Immune deficiency states
Imaging Findings
• “Tramlines” or “honeycombing” represents dilated, thickened
bronchial walls
• Volume loss due to destruction of lung tissue
• Multiple small nodular densities from plugged alveoli
• Signet ring appearance on CT: normally, the vessel is larger than
the corresponding bronchus. In bronchiectasis, the bronchus is larger than the
corresponding vessel
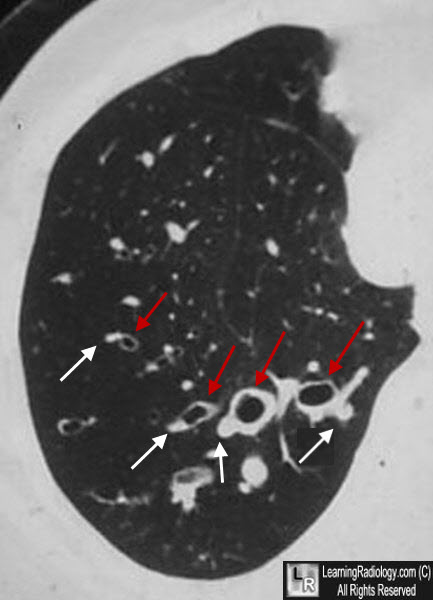
Signet-Ring Sign, Bronchiectasis. The bronchi (red arrows) are larger than their corresponding arteries (white arrows), the reverse of the normal pattern in which the bronchus is smaller than its corresponding vessel.
• Lack of bronchial tapering
• Non uniform bronchial dilation
• Bronchial wall thickening
|
