|
|
Aortic Arch Anomalies
Mirror Image Right Aortic Arch
- General
- Most are asymptomatic
- Unless they cause encircling vascular ring like pulmonary sling
- Can be complex lesions requiring multiple projections
Left Aortic Arch With Anomalous Right Subclavian Artery (RSCA)
- Occurs in less than 1% of people
- RSCA passes posterior to esophagus
- Pushes trachea and esophagus forward
- Produces oblique shadow above aortic arch on frontal film
- Origin of RSCA may be dilated
- Diverticulum of Kommerell is most commonly seen with a right aortic arch and anomalous left subclavian artery (LSCA)
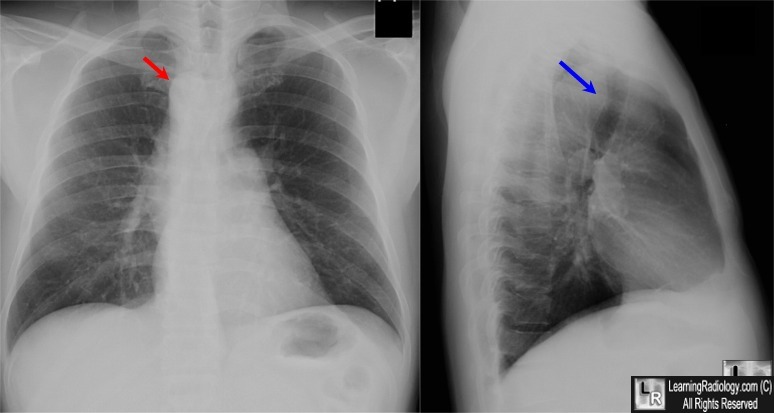
Right Aortic Arch
- Types
- At least five different types
- Only two of importance
- Mirror Image Type — Type I
- Aberrant left subclavian — Type II
- General considerations
- Recognized by leftward displacement of barium-filled esophagus
- Of air-filled trachea
- Aortic knob is absent from left side
- Aorta descends on right
- Para-aortic stripe returns to left side of spine just above diaphragm
- Mirror-image type almost always has associated congenital heart disease (CHD)
- Usually Tetralogy of Fallot
- Aberrant Left Subclavian type rarely has associated CHD
- Most common variety of right arch
Type 1—Mirror Image Type
- Secondary to interruption of left arch just distal to ductus arteriosis
- Associated with congenital heart disease 98% of time
- Imaging Findings
- No posterior impression on trachea or barium-filled esophagus
- Heart is usually abnormal in size or shape
- Aorta descends on right

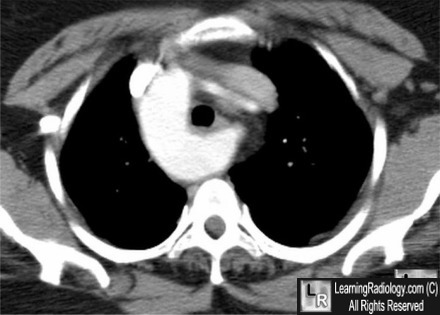
Mirror-image right aortic arch. This contrast-enhanced axial CT scan at the level of the aortic arch
demonstrates a right sided-aortic arch. There is no retrotracheal, retroesophageal
aberrant left subclavian artery. This is the mirror-image variety
with a high association with congenital heart disease..
For a larger photo of the same image, click on this link
Type ll—Aberrant Left Subclavian
-
Secondary to interruption of left aortic arch between LCC and LSC arteries
-
Associated with cardiac defects 5-10% of the time
-
Tetralogy of Fallot most often (71%)
-
ASD or VSD next most often (21%)
-
Coarctation of aorta rarely (7%)
-
Anomalous left subclavian artery (retroesophageal and retrotracheal)
-
Aorta descends on right
-
Imaging Findings -- Right Aortic Arch with Aberrant LSCA
-
If there is a mirror-image right aortic arch, then
-
90% will have Tetralogy of Fallot
-
6% with Truncus Arteriosis
-
5% with Tricuspid Atresia
-
If the person has the following lesions, then the association with a mirror-image arch is
-
Truncus arteriosis 33%
-
Tetralogy of Fallot 25%
-
Transposition 10%
-
Tricuspid atresia 5%
-
VSD 2%
Double Aortic Arch
-
General considerations
-
Most common vascular ring
-
Rarely associated with congenital heart disease
-
Caused by persistence of R and L IV branchial arches
-
Passes on both sides of trachea
-
Joins posteriorly behind esophagus
-
Right arch is larger and higher
-
Left arch is smaller and lower
-
Barium swallow shows bilateral impressions on frontal view
-
Angiogram is characteristic
-
Clinical
-
Anatomy
-
Imaging Findings -- Double Aortic Arch
-
Right arch is higher and larger
-
Left arch is lower and smaller
-
Produces reverse S on esophagram on AP
-
On lateral, arches are posterior to esophagus and anterior to trachea
Cervical Aortic Arch
|
|
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}