|
|
Gastric Volvulus
- Uncommon
- May occur in children due to congenital
diaphragmatic defects
- In adults, rarely occurs before age 50
- Most common cause of gastric volvulus in
adults are diaphragmatic defects
- Stomach twists on itself
- Etiologies
- Abnormality of the suspensory ligaments of the
stomach
- Gastrohepatic
- Gastrosplenic
- Gastrocolic
- Gastrophrenic
- Unusually long gastrocolic and gastrohepatic
mesentery
- Classified as one of two types--organoaxial or
mesenteroaxial
Type |
Appearance |
Description |
Remarks |
Organoaxial |
 |
Twist occurs
along a line connecting the cardia and the pylorus--the luminal
(long) axis of the stomach |
· Most common type.
· Usually associated with diaphragmatic defects.
· Vascular compromise more common. |
Mesenteroaxial |
 |
Twist occurs
around a plane perpendicular to the luminal (long) axis of the
stomach from lesser to greater curvature |
· Chronic symptoms more common.
· Diaphragmatic defects less common. |
- Almost always occur with large diaphragmatic
hernia like hiatal hernia
- Especially, paraesophageal hiatal hernias
- In paraesophageal hernias, gastroesophageal
junction remains in abdomen while stomach ascends adjacent to the
esophagus
- Produces “upside-down-stomach”
- Gastric volvulus is most common complication
of paraesophageal hernias
- Also occurs with eventration of the diaphragm
- Paralysis of diaphragm
- Despite abnormal placement of stomach, it usually
does not become obstructed
- Sometimes called “partial volvulus” or “torsion”
or “chronic volvulus”
- Twisting up to 180 degrees may cause no
obstruction
- Twisting beyond 180 degrees almost always
produces obstruction
- Clinical findings
- Unless acute, patients are frequently
asymptomatic
- When acute and obstructing
- Abdominal pain
- Attempts to vomit without results
- Inability to pass an NG tube
- Together, these three findings comprise the Borchardt triad which is diagnostic of
acute volvulus
- Reportedly occurs in 70% of cases
- Imaging findings
- Massively dilated stomach in LUQ possibly
extending into chest
- Inability of barium to pass into stomach (when
obstructed)
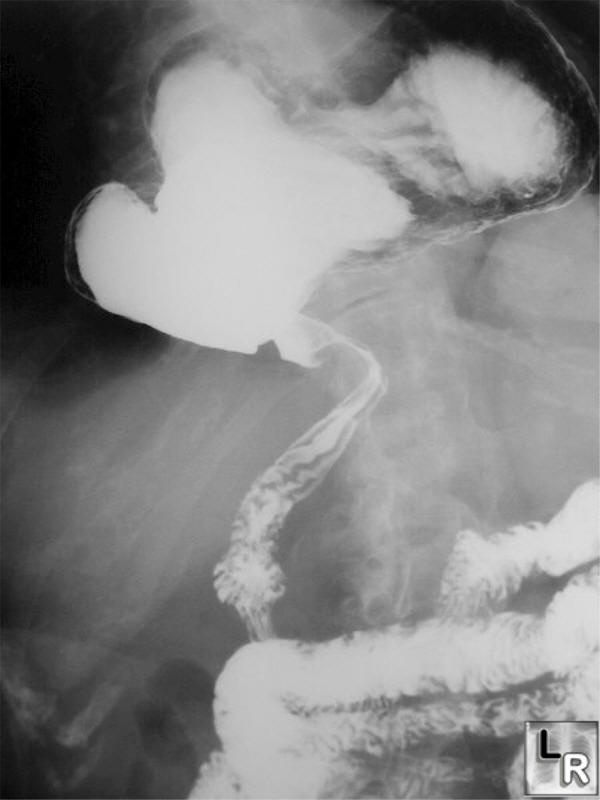
Frontal radiograph from an upper GI examination shows
the stomach
located in the lower chest in a large hiatal hernia. The greater curvature
of the stomach lies superior to the lesser curvature in an organoaxial
twist.
Note that the stomach is not obstructed.

Another frontal radiograph from an upper GI examination again shows
the stomach
located in the lower chest in a large hiatal hernia. The greater curvature
of the stomach lies superior to the lesser curvature in an organoaxial
twist.
Note that the stomach is not obstructed.
- Treatment
- Surgery in acute gastric volvulus
- In patients with chronic gastric volvulus,
surgery is performed to prevent complications
- Nonoperative mortality rate = as high as 80%
- Mortality rate from acute gastric volvulus =
15-20%
- Mortality rate from chronic gastric volvulus
ranges up to 13%
- Complications
- Gastric emphysema
- Twisting of stomach may tear spleen from its
normal attachments
- Perforation is rare
- Margulis and Burhenne-Alimentary Tract Roentgenology
2nd Ed, Vol. 1
- Dahnert 4th edition
- eMedicine Gastric Volvulus by Mohamed Akoad, MD and
Richard Golub, MD
|
|
|
