|
Crohn Disease
Regional Enteritis
Pathology
•
Non-caseating granulomas involved with transmural
inflammation of the
entire GI tract
• Usual age at onset is 15-30, equal male:female ratio
Clinical
• Recurrent episodes of diarrhea
• Occult blood loss and anemia
• Abdominal pain
• Low grade fever
• Anorexia, weight loss
• Perirectal abscess and fistulae
• Malabsorption
• Erythema nodosum and pyoderma gangrenosum
Location
• The maximum length of the involved segment(s) is
determined
at the time
of initial study; i.e. longitudinal
spread is uncommon-except after
surgery
• Esophagus (very rare)
• Stomach (2-20%)
•
Usually involves antrum producing granulomatous
gastritis
• Almost always associated with terminal ileal
disease
• Rams horn sign=poorly distensible, smooth
tubular antrum,
widened pylorus and narrowed bulb
• Aphthous ulcers
• Antral-duodenal fistula
• Duodenum (rare) (4-10%)
• Thickened folds
• Almost never occurs without antral involvement
• Small Bowel (80%) = regional enteritis=terminal ileitis
• Thickening and nodularity of folds
• Aphthous ulcers
• Cobblestone mucosa
• Colon (22-55%) = granulomatous colitis
• Frequently right sided with sparing of rectum
and sigmoid
• Aphthous ulcers with target or bull’s-eye
appearance
• Long, longitudinal fistulous tracts parallel to
bowel lumen
• Colon may be involved without small bowel,
along with small bowel or
become involved after surgery for
Crohn’s
• Rectum (35-50%)
• Sinus tracts
• Deep, collar-button ulcers
Imaging Manifestations
• Squaring of the folds-early manifestation from obstructive lymphedema
• Aphthous ulcers-small nodular filling defects
(mound of edema)
with central ulceration
• Skip lesions-discontinuous involvement of the bowel
with
intervening normal areas
• Proud loops-separation of the loops caused by infiltration
of
the mesentery, increase in mesenteric fat and
enlarged lymph
nodes; simulates a mass
• Cobblestoning-irregular, blanket-like appearance to bowel
wall
caused by criss-crossing longitudinal and transverse
ulcers separated by
areas of edema
• Pseudopolyps-islands of hyperplastic mucosa between
denuded areas of mucosa
• Filiform post-inflammatory polyps
• Pseudodiverticula-from bulging area of normal wall
opposite
side of scarring from disease, usually on
anti-mesenteric side
• String-sign-marked narrowing of terminal ileum (usually)
from a
combination of edema, spasm and (sometimes,
but not always) fibrosis;
frequently associated with proximal dilatation
Differential Diagnosis
•
Ulcerative colitis–continuous
involvement L colon and rectum;
TI normal
• Diverticulitis–tics; intact mucosa; TI normal
• Tuberculosis–but TB has more involvement of cecum,
less of TI
• Radiation ileitis–should have other loops involved and
appropriate hx
• Lymphoma–should have tumor masses, less spasm
• Carcinoid–should have mass; marked fibrosis with
angulation of
loops
• Yersinia– may affect TI but clears in 3-4 months
• Infarction–rare for this location
• Potassium stricture–lacks full clinical picture
• Amebiasis–cone-shaped cecum
Extra-intestinal Manifestations
• Fatty
infiltration of the liver
• Gallstones (28-34%)
• Sclerosing cholangitis
• Bile duct carcinoma
• Amyloidosis
• Urolithiasis:oxalate/uric acid stones
• Migratory arthritis
• Sacroiliitis and ankylosing spondylitis
• Erythema nodosum and uveitis
Complications
• Fistula (33%)
• Fistulae occur more often with regional enteritis than with
granulomatous colitis
• Enterocolic fistulae are mostly between ileum and cecum
• Enterocutaneous fistulae mostly from rectum to skin,
but also to vagina and bladder
• Perineal fistula [Other common causes of
fistula are
iatrogenic and diverticulitis]
• Intramural sinus tracts
• Abscess formation [common]
• Rarely, perforation
• Toxic megacolon (dilated transverse colon with pseudopolyps
in toxic
person=no BE)
• Small bowel obstruction
• Adenocarcinoma (rare)
Prognosis
•
Recurrence rate up to 40% after resection, commonly at
the site of the new terminal ileum and usually within the first
two years post-op
• X-ray demonstration of improvement in regional enteritis
is rare
• Mortality rate of 7% at 5 years and 12% at 10 years after
the first
resection

Crohn Disease of Ileum. There is marked narrowing of the terminal ileum in the right lower quadrant.
The loop sits away from the other small bowel loops ("proud loop") mostly because of surrounding fat.
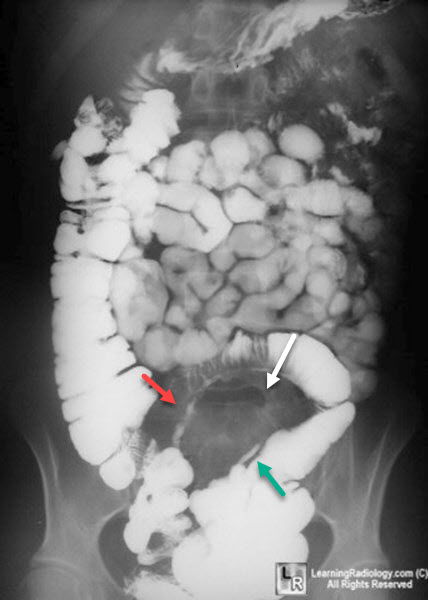
Crohn Disease of Small Bowel. There is marked narrowing of a loop of ileum in the right lower quadrant
(red arrow). The loop sits away from the other small bowel loops ("proud loop") mostly because of surrounding
fat (white arrow). There is a sinus tract also visualized (green arrow), another manifestation of Crohn Disease.
|
