· Defined as the passage of material from the oropharynx into the tracheobronchial tree
· Predisposing conditions include:
§ CNS disorders
§ Intoxication or drug overdose
§ Seizure disorders
§ Recent anesthesia
§ Swallowing disorders
§ Poor oral care
§ Gastroesophageal reflux
§ Esophageal diverticula, such as Zenker’s
· The likelihood of symptomatic aspiration depends in part on the type of material aspirated, the volume aspirated, both of which may be related to the state of consciousness of the individual
· Pattern of disease depends on what is aspirated into lungs
o Un-neutralized gastric acid produces a chemical pneumonitis
§ Known as Mendelson’s Syndrome
§ Can produce near-instantaneous development of airspace disease
§ If massive, the pattern will resemble pulmonary edema
§ Mortality is relatively high (30-60%)
o Aspiration of water or neutralized gastric acid may produce fleeting disease that can resolve in hours
§ Although frequently referred to as a pneumonia, it does not typically produce an infectious response and is not a true pneumonia
o Aspiration of bacteria can produce pneumonia
§ Frequently anaerobic organisms
· Community–acquired infections tend to be caused by Strep pneumoniae, Staph aureus, Haemophilus flu and Enterobacteriaceae
· Hospital-acquired infections tend to be caused by Pseudomonas and other gram-negative organisms
§ Anaerobic infections commonly necrotize, so cavities may be present
· Broncho-pleural fistulae and para-pneumonic effusions or empyema may develop
§ Anaerobic organisms typically produce a longer lasting pneumonia
· Aspiration, no matter what the type, usually occurs in the gravity dependent portions of the lung
§ Lower lobes, especially right-sided, including and especially the superior segments of the lower lobes
· Because of the larger caliber and straighter course of the right main bronchus
§ Posterior segments of the upper lobes
§ Aspiration which occurs while the person is prone may be seen in the right upper lobe and middle lobe or the lingula
· Chronic aspiration pneumonia results from repeated aspiration of foreign material over a prolonged time
o Zenker’s diverticulum
o Achalasia
o TE fistula
o Neuromuscular diseases
o Chronic reflux
o Lipoid pneumonia
§ Mineral oil (used as a laxative)
§ Oily nose drops (not used anymore)
· Clinical findings
o Choking on swallowing
o Acute onset of respiratory distress, if gastric acid
o Slow onset if bacterial pneumonia ensues
§ Low grade fever
§ Productive cough
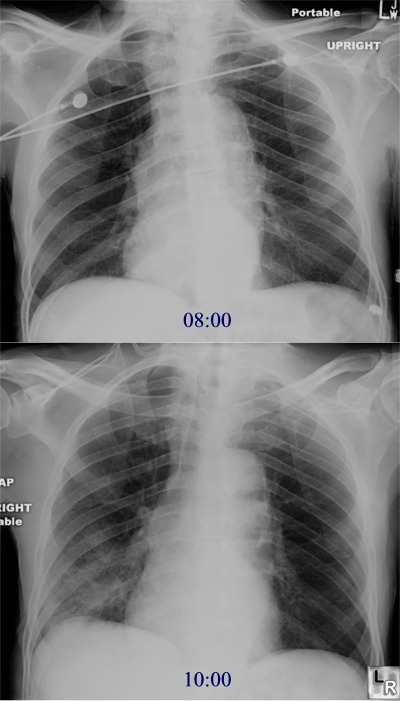
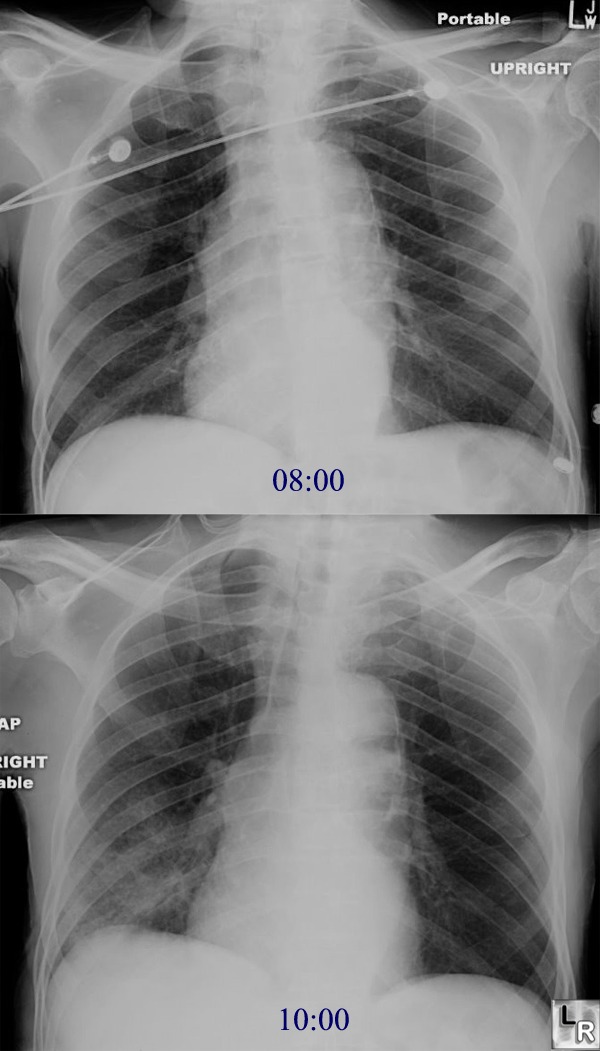
· Imaging findings
o Conventional chest radiography is usually all that is needed to make the diagnosis
o Fleeting infiltrate (lasts less than one or two days) if bland and non-infected
§ Chemical pneumonitis may appear almost instantly while aspiration of bland material may take hours to manifest
§ Pneumonia may not develop fro several days following the incident
o Consolidation of lobe if infected with anaerobic organisms or if aspiration of un-neutralized HCl
o When chronic, the disease usually starts as airspace disease and becomes interstitial as the macrophages incorporate the aspirated material
o May mimic a lung mass when chronic