|
|
Urethral Diverticulum
General Considerations
- Much more common in females than males, in whom they are rare
- Most often in women 30-50 years of age
- In males, they are believed to be congenital; in females, most are acquired
- Relatively common in women, especially with recurrent genitourinary infections, post-void dribbling and dyspareunia
- Described as an outpouching of tissue from the posterior wall of the urethra (usually) into the urethrovaginal potential space
- Lining of diverticulum is identical to urethral mucosa
- Most are thought to be derived from dilated paraurethral ducts or glands
Clinical Findings
- There may be a clinically palpable suburethral mass
- Symptoms include
- Recurrent urinary tract infections (UTI)
- Hematuria
- Urgency
- Early symptoms
- Dysuria
- Frequency
- Post-micturition dribbling
- Later symptoms
Imaging Findings
- Voiding cystourethrography (VCUG) is still probably the imaging study of first choice
- Sometimes, diverticulum fills during voiding phase and is best visualized on post-void film
- Diverticulum will appear as a contrast-containing structure attached to the urethra
- Positive-pressure urethrography (double balloon catheter studies) generally reserved for cases where findings on VCUG are negative but a diverticulum is strongly suspected
- Can be performed with balloons inflated in bladder and at external meatus to “seal urethra” with central portion of catheter filling urethra itself
- Ultrasound, either abdominal, vaginal or endorectal, may also demonstrate urethral diverticula
- MRI has also been used
- T1 shows medium signal intensity, usually homogeneous
- On T2, fluid shows high signal intensity
Treatment
- Treatment is usually recommended if patients are symptomatic
- Surgery is performed and usually involves either: marsupialization, excision or partial ablation, depending on location of the diverticulum
Complications
- In as many as 10% of cases, stones may form within the diverticular sac
- May be multiple
- Usually calcium oxalate or calcium phosphate stones
- May be associated with varying degrees of inflammation (diverticulitis)
- May rupture into space between periurethral connective tissue and the vaginal wall
- Rarely, carcinoma develops within a diverticulum
Prognosis
- Overall cure rate of 70-100% for symptomatic patients

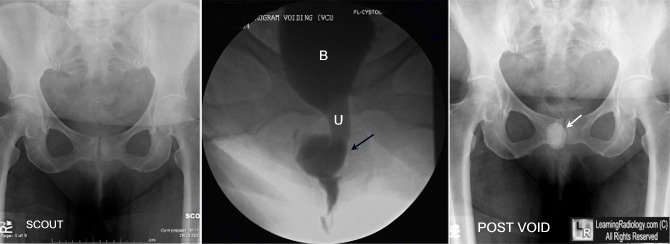
Urethral Diverticulum. Image on left is a scout image before a voiding cystourethrogram (VCUG) was performed. Notice there is no density in the region of the urethra, thus excluding a calcified stone in the urethra. The middle image is from the VCUG showing the bladder (B), the urethra (U) and the mid-urethral diverticulum (black arrow) filling with contrast. The image is reversed so that the contrast appears black on the image. In the image on the right, there is contrast remaining only in the diverticula (white arrow) which fails to empty while the bladder and urethra are free of contrast. In this image, the contrast appears white.
For additional information about this disease, click on this icon if seen above.
For this same photo without arrows, click here
|
|
|

{kind=link}