|
|
Uroepithelial (Transitional) Cell Carcinoma
Submitted by Daniel Kowal, MD
- Accounts for 85-90% of all uroepithelial tumors
- Exophytic, polypoid papillary growth pattern most
common
- Attached to the mucosa by stalk
- Non-papillary tumors less common
- Most
are solid with no characteristic gross findings
- Location
- Bladder is 30-50x more often the site of the tumor than
ureter or renal pelvis (most common tumor of GU tract)
- When it occurs in the ureter, it most commonly occurs in
the lower 3rd
- Synchronous (simultaneous) transitional cell carcinomas
are common
- Bladder involvement with
- 24% of primary renal pelvis involvement
- 30% of primary ureteral involvement
- In 2% with primary bladder tumor
- Both ureters involved in 2-9%
- Both renal pelves in 1-2%
- Metachronous (sequential) transitional cell carcinomas in upper tracts
- With pelvic and ureteral primaries-12% in 25 months
- With bladder primaries-4% (2/3 in 2 years but can
reoccur decades later)
- Most
commonly in men age 60 and older
- Classically present with “painless hematuria”
- Risk
factors
- Exposure to cyclophosphamide
- Phenacetin
- Chronic urinary stasis
- Smoking
- Metastasizes to
- Regional lymph nodes
- Liver
- Lung
- Bone
- Imaging findings
- IVU
- Enlarged and hydronephrotic kidney
- Invasive, poorly
differentiated tumors are more likely to obstruct
- Dilated calyx with
filling defect
- Calyceal amputation
- Partial or complete
obstruction of the infundibulum
- Retrograde studies
- Papillary tumors
- “Goblet” or
“Champagne glass sign” of ureteral dilatation distal
to a filling defect allows for differentiation from
a calculus impacted in the ureter, which causes
distal spasm and narrowing
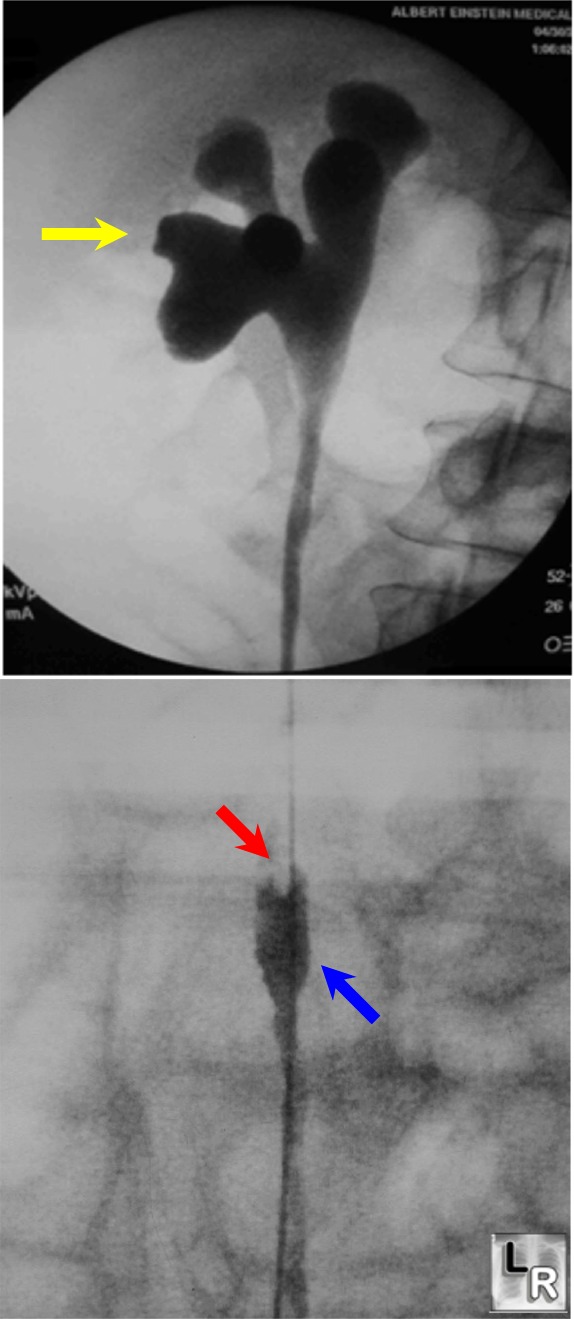
Upper and lower half of right
retrograde pyelogram shows
hydronephrosis (yellow arrow), filling defect at head of
contrast
column in ureter (red arrow) and "goblet" shaped dilatation
distal to filling defect
- Non-papillary tumors
- Nodular or flat
- Cause strictures rather than filling defects
- CT
- Can identify dilated collecting system and demonstrate
level of obstruction
- Intraluminal mass (30-60 HU) representing ureteral tumor
can be differentiated from obstructing calculus (> 190
HU)
- May demonstrate extra-ureteral extension
- US
- Discrete hypoechoic mass within the renal sinus
- Absence of acoustic shadowing allows for differentiation
from calculi
- Angiography
- Hypovascular mass
- Vessel encasement and stain
- Not usually necessary
- Treatment
- Controversy
- Nephroureterectomy with resection of a cuff of bladder versus wide
excision of the tumor alone
- Adding chemotherapy (cisplatin) in patients with
advanced tumors is of unclear utility
|
|
|
