|
Calcified Liver Masses
Ovarian Neoplasms
Calcified Liver Masses - Causes
- Inflammatory
hepatic lesions
- Most
common cause of calcified hepatic lesions
- For
example, granulomatous diseases (tuberculosis).
- Calcification
involves entire lesion
- Appears
as a dense mass
- May
produce artifacts on CT scans
- Echinococcus
cysts have curvilinear or ring calcification
- Central
water density in cyst
- Benign
neoplasms
- Hemangiomas,
especially large ones, may contain large, coarse calcifications; may be
seen at CT in 20% of cases or
radiography in 10%
- Malignant
liver neoplasms
- Hepatocellular adenoma
- Calcifications
may be solitary or multiple
- Usually
located eccentrically within complex heterogeneous mass.
- Fibrolamellar
carcinoma
- Calcifications
reported in 15%-25% of cases at CT
- Occurs
in many patterns
- Intrahepatic
cholangiocarcinoma
- Calcifications
are typically accompanied by a desmoplastic reaction
- Visible
at CT in about 18% of cases.
- Calcified
hepatic metastases
- Most
frequently associated with mucin-producing neoplasms such as colon, or
less likely ovarian, carcinoma
Calcified
Liver Masses - DDX
|
·
Granulomas, as in TB |
·
Hydatid cysts |
·
Hemangiomas |
·
Hepatocellular adenoma |
·
Fibrolamellar carcinoma |
·
Intrahepatic cholangiocarcinoma |
·
Mucin-producing metastases |
|
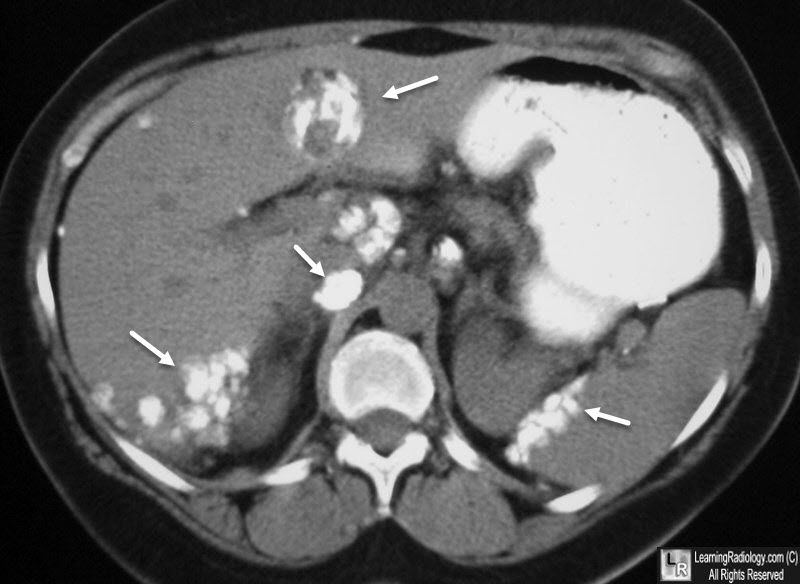
Ovarian Carcinoma Metastases. Calcified liver and peritoneal metastases
from ovarian carcinoma are seen in the liver and along peritoneal surfaces (white arrows).
Ovarian Neoplasms
- Tumors
of Surface Epithelium form 90% of ovarian tumors
- Mucinous Tumors
-
Incidence – 30% of ovarian neoplasms
§
Mucinous cyst adenoma
·
Commonest tumor
·
Age group: 30-50 yrs
·
Bilateral in 10%
§
Mucinous cystadenocarcinoma
·
Age group: 40-60 yrs
·
Bilateral in 10 %
-
Features
§
Large multilocular pedunculated cyst
§
Rare complication may occur with involvement of the peritoneum
·
Pseudomyxoma peritonei (jelly belly)
§
May produce coarse calcifications in primary or
metastases
-
Incidence – 50% of ovarian neoplasms
§
Serous cystadenoma:
·
Age group: 20 – 30 yrs
·
Bilateral in 15%
·
Malignant transformation in 20 – 30 %
§
Serous cystadenocarcinoma:
·
Age group: 40 – 60 yrs
·
Bilateral in 30%
·
5 year survival rate: 30 – 50 %
-
Features:
§
Contain fibrous walled cysts with papillary excrescences
§
Locules contain straw-colored
fluid
§
Psammoma bodies=concentric
calcification in papillary process
·
Usually fine sand-like calcification frequently
difficult to see on plain radiographs
-
Incidence – 20% of ovarian tumors
-
Morphology:
§ Tumors containing solid and cystic areas
§ Filled with hemorrhagic fluid
§ Lined by glandular epithelium
- Clear Cell (mesonephroid tumor)
-
Incidence: uncommon
-
Age group: 50 – 60 yrs
-
Morphology:
§
Unilocular cysts with small cystic spaces
§ Incidence: 1- 2%
§ Occur commonly in perimenopausal women
- Origin : cells derived form oocytes
-
Incidence: 15- 20% of all ovarian tumors, 5% malignant
§
Age: young age
-
Incidence : very common
§
Age : 20 – 20 yrs
-
Bilateral : 10 – 15 %
-
Macroscopic features :
§
Solid tumors, elastic rubbery consistency having
smooth, firm capsule
-
Derived from cells of all three germ layers
-
Types:
§ Mature or benign type (e.g. Dermoid cysts)
§ Immature or malignant
type (e.g. Solid Teratoma)
§ Monodermal or highly specialized (e.g.
Struma
ovarii)
- Choriocarcinoma and Embryonal Cell
Carcinoma
- Choriocarcinoma mostly of placental origin occurs in prepubertal girls. Highly malignant
§
Contains syncytiotrophoblasts and cytotrophoblasts
§ Secretes large quantities of the tumor marker -
HCG
-
Embryonal cell carcinoma
§
Incidence : rare
-
Highly malignant
-
Meig’s syndrome
§
Ascites
§
Right sided effusion
- Primary : 15% - small & large bowel , 20% -
stomach, 6% - breast
- Bilateral smooth surface
- Histologically cellular or myxomatous stroma with
scattered large signet ring cells
·
Routes of Peritoneal Spread
o
Right
subphrenic space
o
The
greater omentum
o
The
Pouch of
Douglas
|
