|
|
Gastric Ulcers
Causes
- Stress
- Burns=Curling ulcer
- Cerebral disease=Cushing ulcer
- Uremia
- Steroid therapy
- Hyperparathyroidism (25% have ulcer disease)
General Considerations
- Multiple in 2-8%
- Coexistent duodenal ulcer disease in 5-42%
- Duodenal to gastric ratio is 3:1
- Multiple postbulbar duodenal ulcers should suggest Zollinger-Ellison Syndrome
Location
- Lesser curvature aspect of body and antrum usually for benign ulcers
- Benign ulcers also occur on posterior wall; not usually anterior wall
- May be found in proximal half of stomach in geriatric patient
- Almost all lesser curvature gastric ulcers <1cm are benign
- Greater curvature benign ulcers are associated with considerable mass effect which erroneously leads to conclusion of malignancy
Imaging Findings of Benign Ulcers
- Two prerequisites for diagnosis of an ulcer
- Ulcer crater-collection of barium on dependent surface which usually projects beyond anticipated wall of stomach in profile (penetration)
- Hampton’s line-1 mm thin straight line at neck of ulcer in profile view which represents the thin rim of undermined gastric mucosa
- Ulcer collar-smooth, thick, lucent band at neck of ulcer in profile view representing thicker rim of edematous gastric wall
- Ulcer mound-smooth, sharply delineated tissue mass surrounding a benign ulcer
- Ring shadow-thin rim of contrast which represents an ulcer on the non-dependent surface of an air-contrast study
- Thickened folds radiating directly to the base of the ulcer en face
Imaging Findings of Malignant Ulcers
- Ulcer projects within the anticipated wall of the stomach
- Ulcer is eccentrically located within the ulcer mound
- Irregularly shaped ulcer crater
- Nodular ulcer mound
- Abrupt transition between normal and abnormal mucosa several cms away from the ulcer crater
- Rigidity, lack of distensibility and lack of changeability
- Associated large mass
- Carmen meniscus sign-a relatively shallow gastric ulcerating malignancy projecting as an ulcer which is always convex inwards to the lumen and which does not project beyond the wall=Kirklin meniscus complex
Healing
- Most gastric ulcers clear completely in 6-8 weeks.
- With healing, ulcer decreases in size and is more likely to appear linear
- Radiating folds become more prominent and extend to crater
- Between 50-90% of healed gastric ulcers produce visible scars on Double Contrast study
Complications of Ulcer Disease
- Bleeding is slightly more common in the duodenum than the stomach
- About 17% of all ulcers are complicated by bleeding
- A filling defect in the ulcer crater may represent a blood clot
- Gastric outlet obstruction is less common than bleeding (5%)
- Stomach may have to be suctioned to get good study
- Benign ulcer disease at the pylorus is a more likely to cause gastric outlet obstruction than cancer
- Perforation in 5-11% is more common in duodenal than gastric ulcers
- Most gastric perforations are from lesser curve ulcers
- Free air is not detected by x-ray in 25-35% of perforated duodenal ulcers
- Penetration is the extension of the ulcer beyond the serosa in to adjacent structures
- Pancreas is most common site, but also biliary tree, colon


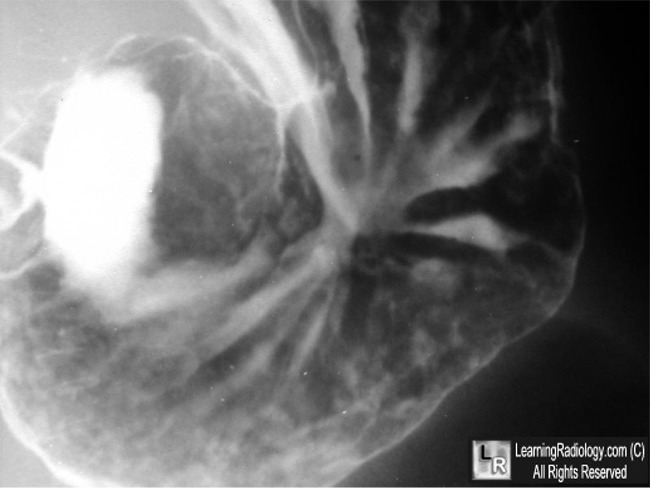
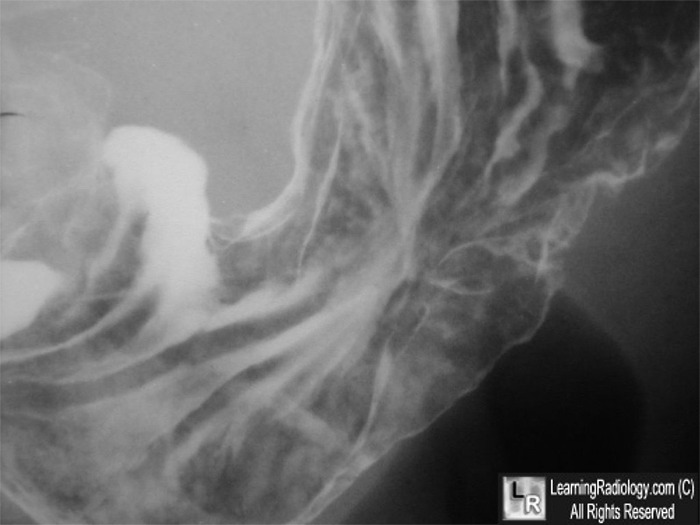
Gastric Ulcer, Benign. Both images are close-ups of the stomach from a double contrast (i.e. air and barium) upper gastrointestinal series. They demonstrate radiating folds (green arrow) coursing to the base of a persistent collection of barium (white arrows) on the posterior wall of the body of the stomach. There is no significant mass effect and the folds radiate right to the base of the ulcer, both signs of benignity.
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
|
|
|

{kind=link}
{kind=link}