|
Intussusception
Submitted by Megan Werner, MSIV
Definition
· Telescoping of a segment of bowel (the intussusceptum)
into another, usually more distal, segment of bowel (the
intussuscipiens)
Etiology/Pathophysiology
· Intussusceptum is pulled further into the distal segment
by peristalsis, pulling the mesentery along with it and trapping the
vessels
· If not reduced, edema, ischemia and bowel obstruction
(usually partial) ensue with necrosis of bowel
· Three etiologies
o Intraluminal
· Intraluminal mass (e.g., pedunculated tumor) is pulled
forward by peristalsis and brings attached bowel wall with it
o Intramural
· Abnormality of bowel wall (e.g., sessile malignancy)
causes it not to contract properly, allowing a kink which serves as a
lead point
o Extraluminal
· Extraluminal factor (e.g., inflamed appendix) causes
area of abnormal peristalsis, allowing a kink which serves as a lead
point
· In children
o Over 90% have no pathologic lead point
· Most thought due to lymphoid hypertrophy following viral
infection
o Less than 10% due to Meckel’s diverticulum, polyp,
lymphoma, etc.
· In adults
o Over 90% have a demonstrable cause
· 60% due to neoplasm (60% malignant, 40% benign)
· 30% due to non-neoplastic abnormalities, such as
inflammation, trauma or suture lines
· 10% are idiopathic
Epidemiology
· In developed nations
· In developing nations
-
Incidence is higher
in adults than it is in developed nations
-
Fewer are associated
with malignancy, and fewer have pathologic lead points
Clinical Findings
· Children
o Cyclical, colicky abdominal pain
o Vomiting
o “Currant jelly” stools (diarrhea with mucus and blood)
or other blood in stool
§ Classic triad occurs in about 1/3 of patients; most have
2 of the 3
o Palpable abdominal mass, often in right upper quadrant
o Dance’s sign: RUQ mass (intussusception) with RLQ empty
space (movement of cecum out of normal position)
· Adults
o Usually indolent, with intermittent crampy abdominal
pain over days to months
o Can be acute obstruction with hours to days of abdominal
distention, pain, and constipation
o Nausea and vomiting
o Tenderness to palpation
o Less than 20% have associated blood in stool
o Rarely have a palpable abdominal mass
o Can be incidental findings if intussusception is
transient and asymptomatic
Imaging Findings
· Plain radiographs are not sensitive or specific
o Children
-
Soft tissue mass
surrounded by a crescent of gas
-
Evidence of distal
small bowel obstruction
-
Absence of or
decreased gas in the colon
-
Pneumoperitoneum
-
May be normal
o Adults usually normal bowel gas pattern
· Barium enema (diagnostic and therapeutic)
- “Coiled spring” appearance
o Barium in lumen of the intussusceptum and in the
intraluminal space
· Ultrasound (not pathognomonic)
o Transverse: Target or doughnut sign, with hypoechoic rim
(edematous bowel wall) surrounding hyperechoic central area (intussusceptum
and associated mesenteric fat)
o Longitudinal: Sandwich, trident or hayfork sign, with
layering of hypoechoic bowel wall and hyperechoic mesentery
o Oblique: pseudokidney sign, with hypoechoic bowel wall
mimicking the renal cortex and hyperechoic mesentery mimicking the
renal fat
o Doppler may help determine viability of the tissue
o Adults: may be less useful, as often cannot identify the
pathologic lead point and is most useful when an abdominal mass is
palpated
· CT (virtually pathognomonic, most commonly done in
adults)
o Transverse
§ Target sign, with layers of fat and bowel wall visible
§ If enhanced may see mesenteric vessels in the layers and
oral contrast in the intraluminal spaces
o Longitudinal
§ Elongated, sausage-shaped mass with visible layers
o May be helpful in judging the degree of vascular
compromise if fluid or gas collections seen in between the walls of
the intussusceptum
o May or may not see any pathologic lead point
Treatment
· NPO, IV fluids, NG tube if gastric distention
· Children
o Surgical consultation
o Then either reduction with barium, hydrostatic (lactated
Ringer’s) or air enema, or surgery
· Adults (best approach debated)
o Colonic: surgical resection without reduction because of
risk of venous embolization of tumor or seeding from a malignant tumor
o Enteroenteric: depends on
cause and symptoms; may require resection or manual reduction during
surgery, may be treated with enema reduction, or may require no
intervention
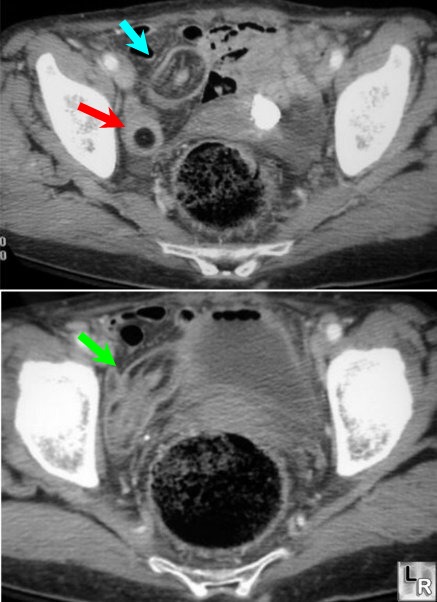
Two images from a CT of the abdomen and pelvis show a lipoma of the
ileum (red arrow)
which serves as the lead point for the intussusception shown by the
target sign (blue arrow)
and a longitudinal view of the intussusception showing the sausage
shaped mass (green arrow)
|
