|
|
Esophageal Varices
- Dilated submucosal veins due to increased collateral blood flow from portal venous system to azygos system
- Uphill varices
- Collateral blood flow from portal vein via azygos vein into SVC (usually lower esophagus drains via left gastric vein into portal vein)
- Most common cause is portal hypertension secondary to cirrhosis
- Varices in lower half of esophagus to the level of the carina (azygos vein)
- More common than downhill varices
- Causes
- Intrahepatic obstruction from cirrhosis
- Splenic vein thrombosis (usually gastric varices only)
- Obstruction of hepatic veins
- Portal vein thrombosis
- IVC obstruction below hepatic veins
- Marked splenomegaly / splenic hemangiomatosis (rare)
- Downhill varices
- Collateral blood flow from SVC via azygos vein into IVC / portal venous system (upper esophagus usually drains via azygos vein into SVC)
- Varices in upper 1/3 of esophagus
- Usually extend down to the level of the carina (azygos vein)
- Less common than uphill varices
- Causes
- Obstruction of superior vena cava distal to entry of azygos vein due to
- Lung cancer (most common)
- Lymphoma
- Retrosternal goiter
- Thymoma
- Mediastinal fibrosis
- Imaging Findings
- Small amount of barium (not to obscure varices)
- Relaxation of esophagus (not to compress varices)
- Refrain from swallowing because each succeeding swallow initiates a primary peristaltic wave that lasts for 10-30 seconds
- Sustained Valsalva maneuver precludes swallowing
- In LAO projection with patient recumbent or in Trendelenburg position
- Plain film
- Lobulated masses in posterior mediastinum (visible in a small percentage of patients with varices)
- Silhouetting of descending aorta
- Abnormal convex contour of azygoesophageal recess
- UGI
- Thickened and interrupted mucosal folds (earliest sign)
- Tortuous radiolucencies of variable size and location
- "Worm-eaten" smooth lobulated filling defects
- Findings may be accentuated after sclerotherapy
- CT
- Thickened esophageal wall and lobulated outer contour
- Scalloped esophageal luminal masses
- Right- / left-sided soft-tissue masses = paraesophageal varices
- Marked enhancement following dynamic CT
- Complications
- Bleeding in 28% within 3 years
- Exsanguination in 10-15%
- DDx
- Early
- Other forms of chronic esophagitis
- Late
- Varicoid carcinoma of esophagus
- Wall more rigid and less likely to change in varicoid carcinoma
- Nodular filling defects in varicoid ca
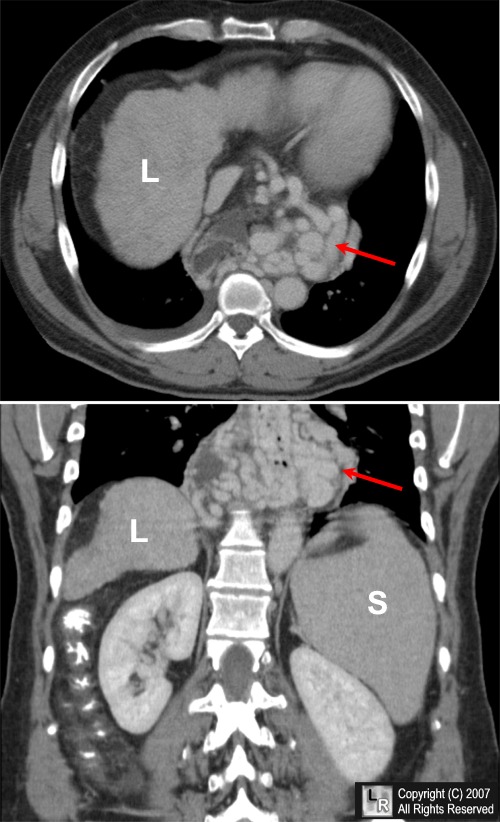
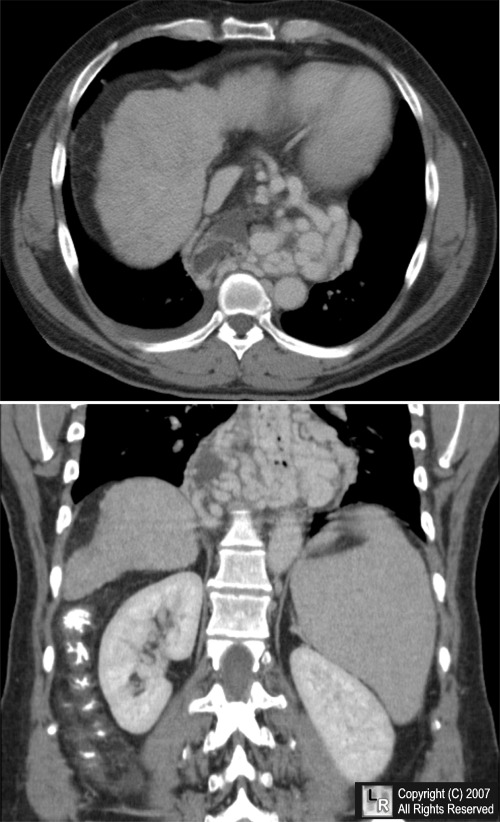
Esophageal varices. An enhanced axial (top) and coronal reconstruction CT scan of the upper abdomen shows markedly tortuous and dilated varices surrounding the lower esophagus. The liver (L) is small and nodular from cirrhosis and the spleen (S) is enlarged from portal hypertension.
For additional information about this disease, click on this icon if seen above.
For this same photo without the arrows, click here
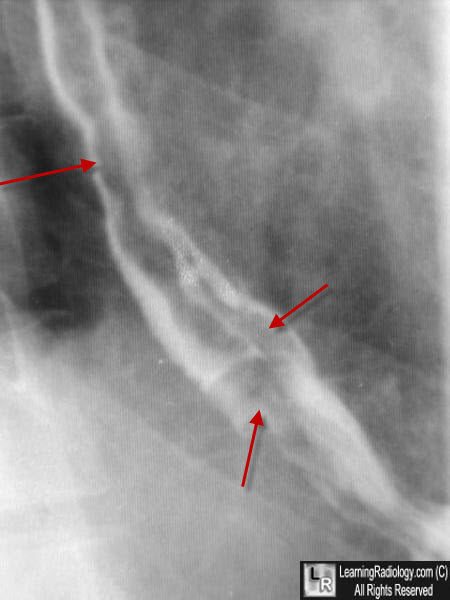
Esophageal varices. Close-up of the lower esophagus during a barium swallow shows multiple serpiginous filling defects in the barium column (red arrows) from varices protruding into the lumen from the wall.

Esophageal varices. Close-up of the lower esophagus during a double-contrast barium swallow shows multiple serpiginous filling defects in the barium column from varices protruding into the lumen from the wall.
Practical Alimentary Tract Radiology 1993
|
|
|

{kind=link}