|
Duodenal Ulcer
General Considerations
•
2-3 times more frequent than gastric ulcers
•
3:1 male:female ratio
Pathophysiology
•
Excessive acidity in duodenum from
• Abnormally high gastric secretion
• Inadequate neutralization
Predisposing factors
•
Steroids
•
Severe head injury
•
Post-surgical
•
COPD
Location
• Bulbar (95%)
• Anterior wall–
50%
• Posterior wall–
23%
• Inferior fornix–
22%
• Superior fornix–
5%
• Postbulbar (3-5%)
• Majority on medial wall just proximal to ampulla
• Tendency for hemorrhage in 66%
• Male:female ration 7:1
X-ray
•
Small round, ovoid or linear crater
• Kissing ulcers–ulcers opposite
from each other on the anterior and posterior walls
• Giant duodenal ulcer–>3cm
(rare) with higher morbidity and mortality
• May be mistaken for the duodenal bulb itself and missed
• Clover-leaf deformity–healed
central ulcer of the bulb with four-leaf clover-like deformity remaining
Complications
•
Hemorrhage 15% melena>hematemesis
•
Perforation
<10% anterior>posterior /may fistulize to GB
•
Obstruction
5%
•
Penetration <5% walled-off
perforation
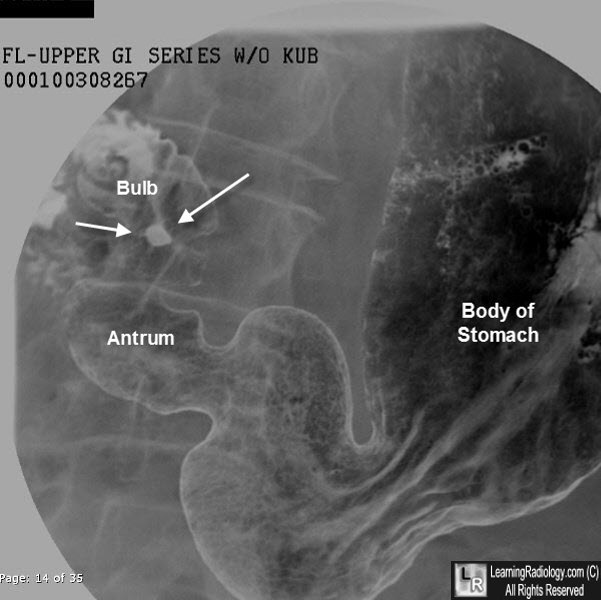
Duodenal Ulcer. There is a collection of barium on the dependent surface of the duodenal bulb (white arrows) on this double contrast (air-contrast) upper GI examination. This represent barium in an ulcer crater.
|
