|
|
Carcinoma of the Colon
Risk Factors
- Adenomatous polyp
- Family history of benign or malignant colon tumors
- Chronic ulcerative colitis
- Crohn’s disease
- Prior pelvic radiation
- In women who have carcinoma of breast or uterine ca
- Retinitis pigmentosa
- Familial polyposis
- Gardener’s syndrome
- For synchronous lesions=1% (two or more colon ca’s at same time)
- For metachronous lesions=4-5% (likelihood of a person with colon ca developing 2nd)
Pathology
- Adenocarcinomas make up the vast majority
- Squamous cell carcinoma can start at the anal verge
- Cloacogenic carcinoma spreads mostly by direct invasion
Clinical Findings
- Peak age 50-70 years
- Weight loss
- Blood in stool
- Loss of appetite
- Change in bowel habits
Location
- Rectum (15%), sigmoid (20%), descending colon (10%), transverse colon (12%), ascending colon (8%), cecum (8%)
- Location seems to be changing and moving back to cecum
- More common in right colon with advancing years
- More common in left colon with chronic ulcerative colitis
Imaging findings
- 90-95% rate of detection by BE
- Polypoid filling defect
- Annular constricting=apple-core lesion
- Scirrhous ca-rare infiltrating type which gives lead-pipe appearance seen especially in ulcerative colitis
- Calcifications-rare
- May have retrograde without antegrade obstruction
Mets to colon
- Stomach, breast, pancreas, and GU pelvic malignancies via blood
- May also spread via intraperitoneal seeding, especially from ovary
Complications
- Obstruction-antegrade/retrograde or both
- Perforation is relatively common
- Carcinomas of the transverse colon can spread via direct extension to stomach
- Intussusception of lesions in TI or cecum
- Ischemic colitis may occur if chronic obstruction
Metastases from Colon Cancer
- Liver (25%)
- Retroperitoneal and mesenteric nodes (15%)
- Hydronephrosis (13%)
- Adrenal (10%)
- Ovarian mets
- Ascites
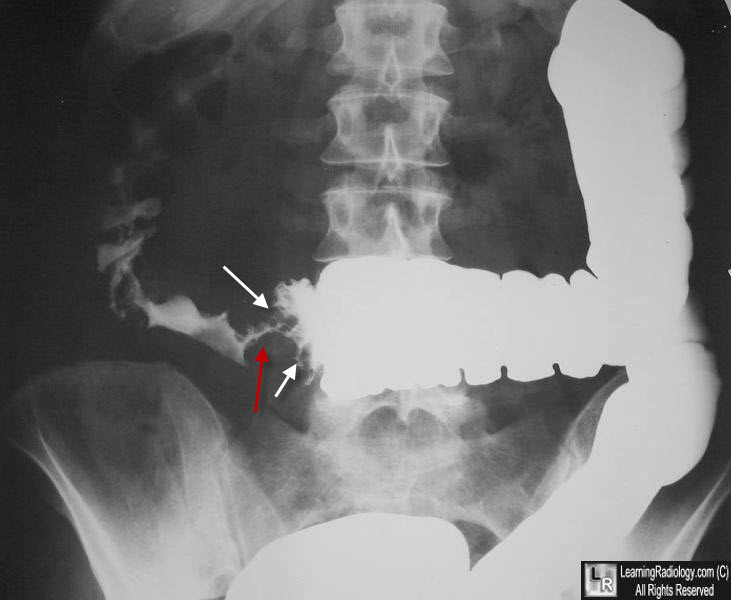
Colonic Carcinoma, Apple-Core Sign. An encircling mass in the mid-transverse colon (red arrow) mostly obstructs the retrograde flow of the barium in this single-contrast barium enema. The shelf-like defect caused by the distal end of the mass (white arrows) produces half of the "apple-core" sign of colon carcinoma.
|
|
|
