|
|
Mediastinal Teratoma
Dermoid
- Mediastinum is a
rare site for occurrence of teratomas, most being ovarian in origin
- Arise from
primitive germ cell rests
- Supposed to
migrate along urogenital ridge to primitive gonad
- Journey is
interrupted in the mediastinum
- May be solid or
cystic
- Three
major categories
- Mature teratomas
- Well-delineated from surrounding tissues
- Contain ectodermal elements along with cartilage, fat and smooth
muscle
- Immature teratomas
- Same elements as above with primitive tissues found in fetus
- Teratomas with malignant transformation
- Overall about 30% are malignant
- Usually adenocarcinoma in mature teratomas
- Angiosarcoma or rhabdomyosarcoma in immature teratomas
- Most of the cystic lesions are benign and most of the solid lesions are
malignant
- Both occur
early in life—young adults most commonly
- DDX from
thymomas which usually occur in 5th or 6th decade
- Clinical Findings
- Usually
asymptomatic
- Large lesions
can cause shortness of breath, cough or retrosternal pain or fullness
- Rare rupture of
dermoid into trachea which leads to trichoptysis—expectoration
of hair
- Associations
- Non-lymphocytic
leukemia and malignant histiocytosis with immature teratomas
- Imaging findings
- Most occur in
the anterior mediastinum, near junction of great vessels and
heart
- Benign lesions are usually smooth in contour whereas malignant
masses tend to be lobulated
- Usually larger than thymomas
- Calcification
may rarely occur but is of no
help since thymomas also calcify
- Exception
would be the very rare occurrence of a tooth or bone in a dermoid
- CT shows fatty
mass with globular calcifications and rarely a tooth or bone
- Fat-fluid
level may be seen on CT
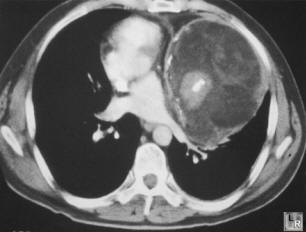
Mediastinal Teratoma. Enhanced CT scan of the chest shows large, septated
anterior
mediastinal mass containing fat and bony elements
- Rapid increase in
size may mean hemorrhage into a cyst rather than enlarging malignancy
- Treatment and
prognosis
- Mature teratomas
- For benign
cystic teratomas, surgical resection
- Excellent
prognosis
- Immature
teratomas
- In childhood,
surgical excision is often successful
- In adults,
tend to have a more malignant course
- Teratomas with
malignancy
- Usually highly
aggressive
- Poor prognosis
- Teratoma versus
dermoid
- Dermoid contain only epidermis
- Teratomas contain all 3 germ layers, but are mostly endodermal when
malignant
- Other germ cell
neoplasms
- Benign dermoid cysts
- Benign and malignant teratomas
- Seminomas
- Choriocarcinomas
- Embryonal cell carcinomas
- Mediastinal seminomas
- Rare
- Almost always in
young men
- Identical to
testicular seminoma and ovarian dysgerminoma
- May be well-encapsulated or invasive
- Tends to be lobulated
- Cannot be
differentiated from teratoma
- Primary choriocarcinoma
- Even rarer than
seminoma in the mediastinum
- Only 23 reported
in the literature, almost all in men
- Occur between
20-30 years
- May be lobulated
- May have
elevated beta sub unit of HCG
- Growth is very
rapid leading to dyspnea, hemoptysis, stridor
- Gynecomastia and
a + Aschheim-Zondek test can occur
- Rapidly fatal
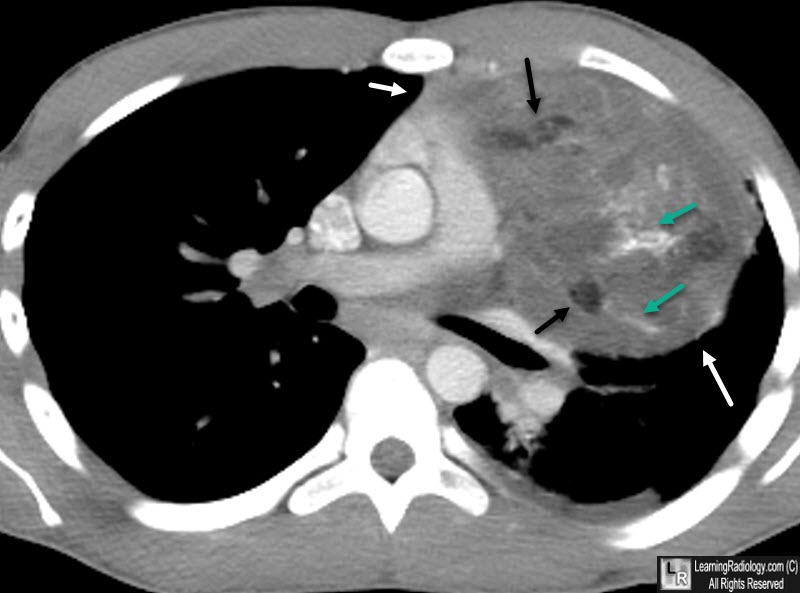
Mediastinal Teratoma. A large anterior mediastinal mass (white arrows) is seen on this contrast-enhanced CT of the chest. The mass contains low density fat (black arrows) and calcifications (green arrows) consistent with a teratoma.
Fraser and Pare
|
|
|
