|
|
Pneumoconiosis
Silicosis
-
Exposure
to silica from mining of coal, graphite, iron,
tin, uranium, gold, silver,
copper
-
After
silica particles are ingested by alveolar macrophages,
breakdown of
macrophage releases enzymes which produce
fibrogenic response
-
Silicosis has a progressive nature despite
cessation of dust exposure
-
Imaging
picture is of multiple small rounded opacities
-
Usually
in the upper lobes
-
May
occasionally calcify (20%)
-
Lymph node enlargement is common
-
Large
opacities are conglomerations of small opacities
-
Progressive
Massive Fibrosis (PMF)
Cavitate
from tuberculosis or ischemic necrosis
-
Eggshell
calcification of hilar nodes in 5%
-
Caplan’s
syndrome consists
of large necrobiotic nodules
superimposed on silicosis
-
Silicosis predisposes to TB
Coal Workers’ Pneumoconiosis (CWP)
-
Originally
silica was erroneously thought to be the cause of CWP
-
Actually
mostly due to the inhalation of
pure carbon
-
Still
referred to as anthrosilicosis or anthracosis although
most coal in USA is
bituminous
-
Coal
dust is deposited in the alveolar macrophages which
migrate to, and leave,
coal dust deposits around the
respiratory bronchiole
-
Complicated
CWP occurs as large masses in
either the upper
lobes or the superior segments of the lower lobes
-
Unlike
silicosis, the large upper lobe lesions of CWP are
single (rather than
conglomerate) black masses with a liquid
core,
not a fibrous tissue core
-
The
masses may undergo cavitation
either from TB or ischemia
-
The
rounded opacities of CWP, found predominantly
in the upper lobes
-
Do
not progress in the absence of more coal dust
-
Classification
is by the International Labor Organization’s
1980 classification (p,q,r,
etc.)
-
There
is a direct correlation between the amount of coal
dust contained in the
lungs and the profusion category
Asbestosis
-
Salts
of salicic acid
-
90%
of asbestos in the USA is white asbestos (chrysotile)occurs in automotive workers, shipfitters,
construction workers
-
Asbestos
particles invoke a hemorrhagic response in the lung
-
Affects
lower lobes first
-
Opacities
are small and irregularly shaped
-
Cardiac
silhouette may
become shaggy
-
Almost
all patients have some pleural involvement-pleural
plaque, diffuse pleural
thickening, calcification or effusion
-
Pleural
involvement without parenchymal disease is common
-
Parietal
pleural plaques in the mid lung are the most common
asbestos-related
disorder and are usually bilateral
-
Pleural calcification occurs in about 50% with asbestos-related
disease, especially diaphragmatic pleura
-
Diffuse
pleural thickening involves diaphragmatic pleura, blunting
of costophrenic
sulci and lateral chest wall thickening
- Effusion
alone may occur early in the disease
(first 20
years) in about 3% of cases
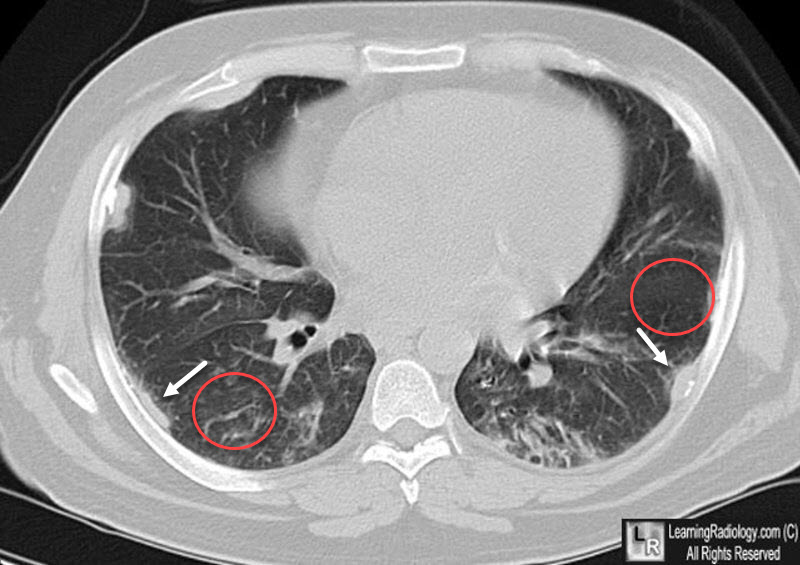
Asbestosis. There are multiple pleural plaques, some calcified, some not (white arrows). There are also small, irregularly-shaped desnities in the lung parenchyma (red circles)
-
Asbestos-related
lung cancer is either squamous
cell or adenocarcinoma
-
Bronchogenic
ca is almost always associated with cigarette smoking
-
Mesotheliomas most often due to crocidolite particles
-
Mesotheliomas are not related to cigarette smoking
-
In
contrast to silicosis, hilar lymph
nodes are rarely affected
|
|
|
