|
|
Sternomanubrial Dislocation
General Considerations
- Rare
- Usually occurs with high energy impact, such as motor vehicle accidents
- Can occur with lower impact forces if there is a pre-existing arthropathy, e.g. rheumatoid arthritis or severe kyphosis
- Joint may be synovial (dislocation most common), synchondral, or synosteal (latter two typically fracture through manubrium without dislocation)
- Types
- Type 1—body of sternum dislocated posteriorly with respect to the manubrium
- Usually caused by direct impact to sternum
- More often associated with other traumatic abnormalities
- Type 2-- manubrium dislocated posteriorly with respect to the body of sternum
- Due to hyperflexion of the upper thoracic spine transmitting downward and posterior force to manubrium through first ribs
Clinical Findings
- Suspected clinically
- Instability
- Deformity
- Severe pain over sternomanubrial junction
Imaging Findings
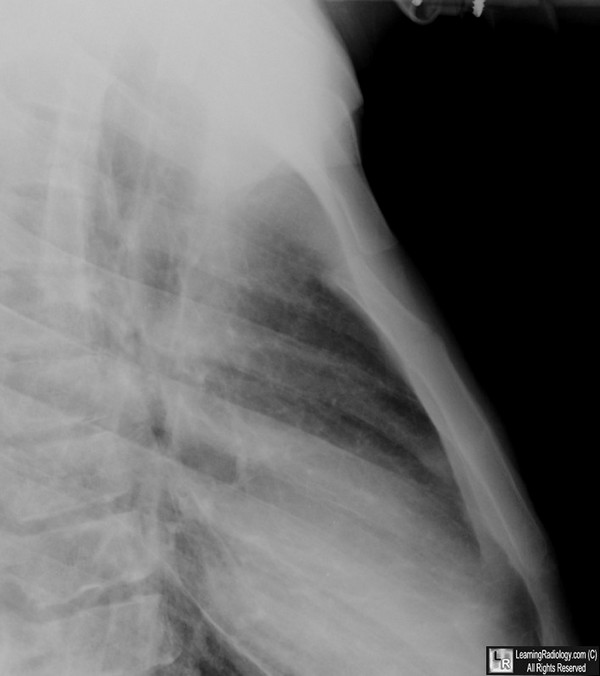
- Frontal radiograph of the chest is rarely diagnostic
- Lateral chest radiographs or CT scans confirm diagnosis
- On CT, other potentially life-threatening injuries to aorta, great vessels, trachea, and esophagus may be seen
- Upper thoracic spine and rib fractures share the hyperflexion mechanism of type 2 sternomanubrial injuries
Treatment
- Depends on stability of injury and presence of associated injuries
- Stable, uncomplicated injuries are treated with closed reduction
- Unstable injuries and those with an associated mediastinal injury may require open reduction

Sternomanubrial Dislocation. Close-up of a lateral chest radiograph shows
posterior dislocation of the body of the sternum (red arrow) relative to the manubrium (white arrow)
at the sternomanubrial joint.
For this same photo without the arrows, click here
For more information, click on the link if you see this icon 
Traumatic Sternomanubrial Dislocation with Associated Bilateral Internal Mammary Artery Occlusion. SG Cheng, DJ Glickerman, R Karmy-Jones and JJ Borsa1. AJR March 2003 vol. 180 no. 3 810
|
|
|

{kind=link}