|
|
Dislocations of the Shoulder
Posterior Shoulder Dislocation
- Types of dislocations about the shoulder
- Glenohumeral dislocation (the most common by
far)
- Acromioclavicular dislocation (12%)
- Sternoclavicular dislocation (uncommon)
- Types of glenohumeral dislocations
- Anterior or subcoracoid shoulder dislocation (96%)
- Mechanism
- External rotation and abduction
- 40% recurrent
- Age
- May be associated with:
- Fracture of greater tuberosity (15%)
- Bankart lesion
- Fracture of anterior glenoid rim
- Hill-Sachs defect (50%)
- Impaction fracture of posterolateral
surface of humeral head due to impaction of humeral head against
anterior rim of glenoid during dislocation
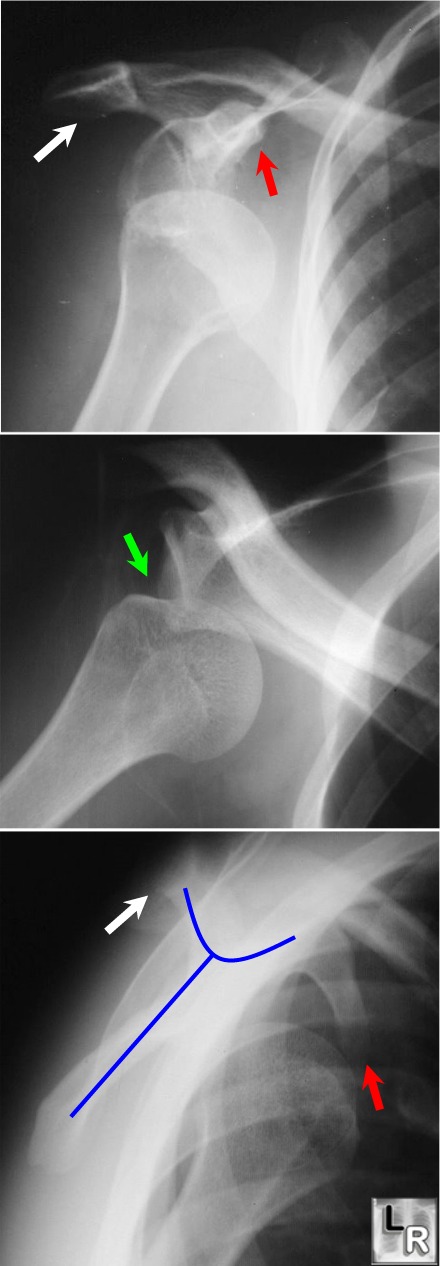
Anterior
Dislocation of the
Humeral Head: Top image shows
humeral head displaced
from glenoid
and lying inferior to
the coracoid process
(red arrow); the
middle image
demonstrates a defect
along the
posterolateral aspect
of the head, which is
the Hill-Sach's
deformity (green
arrow). The lower
image is the scapular
Y view (blue line
outlines scapula). The
head lies in a
subcoracoid (i.e.
anterior location). The white arrows point
to the acromion.
- Posterior shoulder dislocation (2-4%)
- Causes
- Traumatic
- Convulsive disorders or electroshock
therapy
- Nontraumatic
- Congenital or developmental
- May be done voluntarily, especially in
children
- Usually due to axial loading of an adducted
and internally rotated arm
- In >50% unrecognized initially and
subsequently misdiagnosed as frozen shoulder
- May be difficult to see on AP radiograph
- Typically, a scapular Y view or
transthoracic lateral of the humeral head demonstrate a posterior
dislocation better
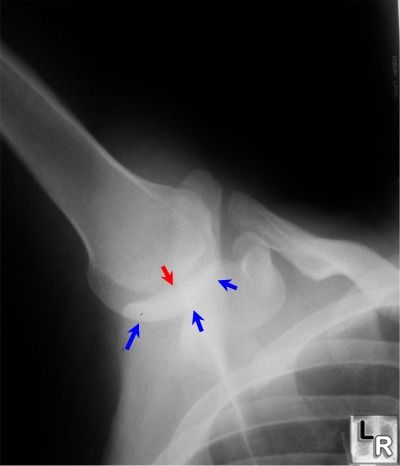
- Imaging signs of posterior dislocation
- Rim sign (66%) = distance between
medial border of humeral head and anterior glenoid rim >6 mm
- Humeral head is fixed in internal rotation
no matter how forearm is turned – “lightbulb sign”
- May be associated with:
- Trough sign (75%) = "reverse
Hill-Sachs" = compression fracture of anteromedial humeral head
- Fracture of posterior glenoid rim
- Avulsion fracture of lesser tuberosity
- Isolated fractures of the lesser
tuberosity should raise suspicion of an associated posterior
dislocation
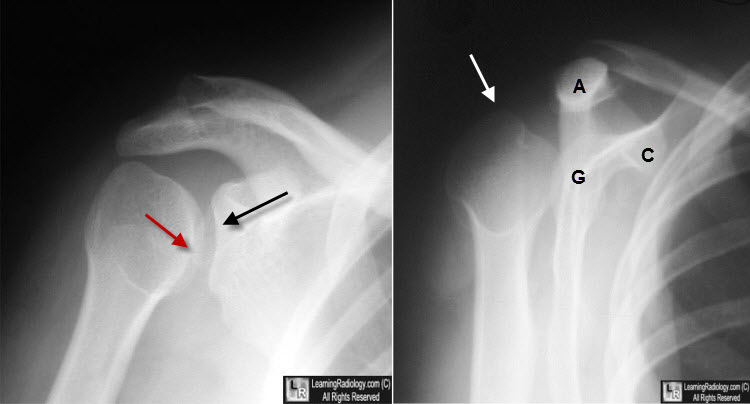
Posterior Dislocation of the Shoulder. Image on left demonstrates a "trough fracture" or "reverse Hill-Sachs fracture"of the antero-medial aspect of the humeral head (red arrow) as well as widening of the glenohumeral joint space (black arrow). The scapular Y view on the right shows that the humeral head (white arrow) no longer resides in the glenoid (G) but posterior to the acromion (A), The coracoid process is marked C.
- Inferior shoulder dislocation (1-2%)
- Luxatio erecta
- Extremity held over head in fixed position
with elbow flexed
- Mechanism
- Severe hyperabduction of arm resulting in
impingement of humeral head against acromion
- Humeral articular surface faces inferiorly
- Complications
- Rotator cuff tear
- Fracture of acromion with or without inferior
glenoid fossa and with or without fracture of the greater tuberosity
- Neurovascular injury
Luxatio Erecta (Inferior Dislocation). The humeral head (white arrow) lies below (inferior) to the
glenoid (black arrow) and the arm is fixed in abduction.
- Superior shoulder dislocation (<1%)
- Humeral head driven upward through rotator cuff
- May be associated with fracture of humerus,
clavicle or acromion
|
|
|
