
Recognizing A
Pleural Effusion
© William Herring, MD, FACR
Normal Anatomy
Visceral pleura is adherent to the lung
Space between visceral and parietalpleura is a potential space
Infoldings of visceral pleura formfissures
Loose connective tissue beneathvisceral pleura = subpleural space
Normal Physiology
Normally there are 2-10 cc of fluid inthe pleural space
Each hour, as much as 100cc of fluid isproduced, mostly at parietal pleura
Fluid drains mostly to visceral pleuraand via lymphatics
Abnormal Physiology
Pleural effusions may form when
Increased hydrostatic pressure
Decreased colloid osmotic pressure
Increased capillary permeability
Decreased absorption of fluid by lymphatics
Decreased pressure in pleural space
Transport of peritoneal fluid through diaphragmor via lymphatics
Pleural Effusion-Types
Transudate
Exudate
Empyema
Hemothorax
Chylothorax
Transudate
Increased capillary hydrostatic pressureor decreased osmostic pressure
CHF
Hypoalbuminemia
Cirrhosis
Nephrotic syndrome
Exudate
Usually secondary to neoplastic orinflammatory dzs involving pleura
[Fluid Protein] / [serum protein] > 0.5
[Fluid LDH] / [serum LDH] >0.6
Fluid LDH > 2/3 highest normal serumLDH
Specific Types of Effusions
Hemothorax
Fluid hematocrit > 50% blood hematocrit
Empyema = exudate containing pus
Chylothorax = increased triglyceridesor cholesterol
Obstruction or rupture of lymphatic vessels
Side-specificity
Mostly left-sided
Pancreatitis
Dressler’s syndrome
Distal thoracic duct obstruction
Mostly right-sided
Heart failure
Abdominal disease related to liver or ovary
Proximal thoracic duct obstruction
Appearances of Pleural Effusions
Subpulmonic effusion
Blunting of Costophrenic angle
Meniscus sign
Layering
Loculated
Laminar effusion
Opacified hemithorax
Air-fluid levels
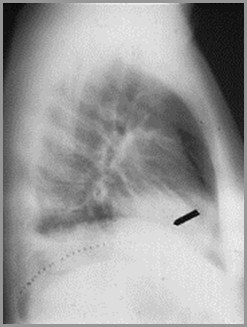
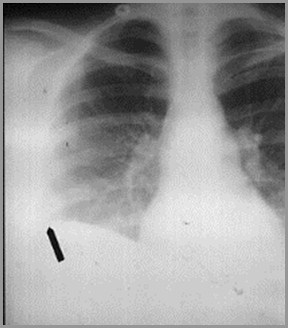
Subpulmonic Effusion
Usually less than 300-350cc
Accumulates at base of lung betweenvisceral and parietal pleura
Causes apparent lateral displacement ofhighest part of hemidiaphragm
Flat-edge sign on lateral
Increased distance between stomachbubble and base of lung
Subpulmonic Pleural EffusionOn the frontal film, the highest point of the apparent right hemidiaphragmis displaced laterally (it is usually in the center). On the lateral film, thereis a flat edge where the effusion meets the major fissure
Blunting of the CP Angle
Normally there are 2-10cc of fluid in thepleural space
When >75cc accumulate, the posteriorcostophrenic (CP) sulci, seen on thelateral film, become blunted
When 200-300cc accumulate, the CPsulci on the frontal film become blunted
When 200-300cc of fluid accumulate in pleural space, the usually acutecostophrenic angle (sulcus), as seen on the right in this person,becomes blunted (as seen on the left in this person)
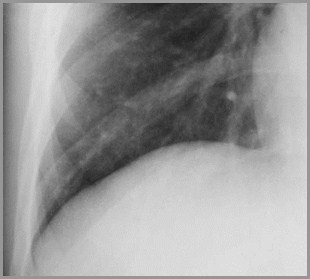
Normal R costophrenic angle
Blunted L costophrenic angle
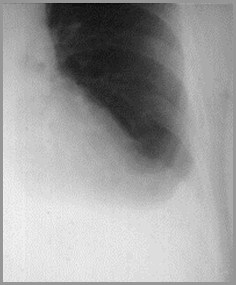
Meniscus Sign
Pleural fluid tends to rise higher along itsedge producing a meniscus shapemedially and laterally
Usually only lateral meniscus can be seen
The meniscus is a good indicator of thepresence of a pleural effusion
Meniscus Sign

Fluid rises higheralong the edge ofa pleural effusionproducing anupside down “U”or meniscusshape
Effect of Position - Layering

Supine
Erect
In the supine position, the fluid layers out posteriorly and produces ahaziness, especially near the bases (since the patient is actually semi-recumbent). In the erect position, the fluid falls even more to the bases.
Loculated Effusion
Occurs secondary to adhesions whichform between visceral and parietal pleura
Adhesions more common with blood(hemothorax) and pus (empyema)
Loculated effusions have unusual shapesor positions in thorax
E.g. remain at apex on erect films
Loculated Effusion
A loculated effusionhas an unusualshape (lentiform) orposition in thethoracic cavity
This is a loculatedempyema
Laminar Effusion
A laminar effusion collects in the looseconnective tissue between the lung andthe visceral pleura
It is not usually free-flowing
It usually occurs with CHF orlymphangitic spread of malignancy
Laminar Effusion

A laminar effusion collectsbetween the lung and thevisceral pleura in the looseconnective tissue of thesubpleural space
Laminar effusions areusually seen with CHF orlymphangitic spread oftumor
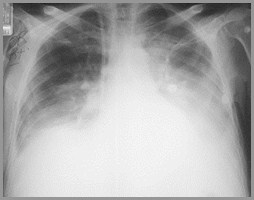
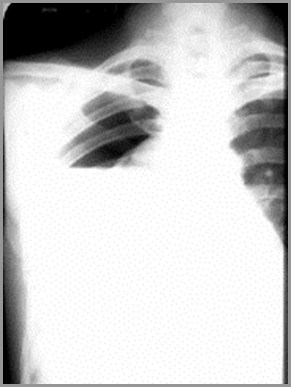
Opacified Hemithorax
If an effusion fills the entire hemithorax, itacts like a mass
There is displacement of the heart andtrachea away from the side of opacification
In atelectasis of an entire lung, the heartand trachea are pulled toward the side ofopacification

The righthemithorax isopaque
There is a shift ofthe heart andtrachea away fromthe side ofopacification
This ischaracteristic of apleural effusion
Large Right Pleural Effusion
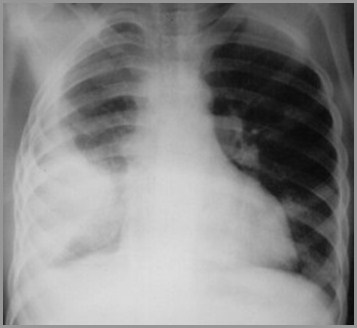
Hydropneumothorax
If both a pneumothorax and a pleuraleffusion occur together, it is called ahydropneumothorax
A hydropneumothorax is usually due totrauma, surgery, bronchopleural fistula
It is characterized by an air-fluid level inthe hemithorax
Hydropneumothorax
A straight edge,indicative of a fluidinterface, in thiscase an air-fluidinterface, is seen onthe right.
In order to have anair-fluid level in thepleural space, theremust be apneumothoraxpresent.
Take Home Points
Pleural effusions are transudates orexudates
It takes from 200-300cc to blunt thecostophrenic sulcus on the frontal view
The meniscus is the classic shape of aneffusion on a frontal film
Pleural effusions shift the mediastinalstructures away from the side opacified

Congratulations, You Graduate

You know youreffusions when yousee them