22 “Must See” DiagnosticImages for MedicalStudents
© Copyright William Herring, MD, FACR
All images retain the copyrights of their original authors
Index at end of presentation
AMSER’s “Shortlist”
•AMSER is the national Alliance of Medical StudentEducators in Radiology
•Their National Curriculum for Medical Students,developed by Kitt Shafer, MD and Petra Lewis, MD,contains a “Diagnostic Shortlist” of “must see" images“all students should recognize”
•This is a limited list of diagnoses that AMSER believesall students should be able to recognize, regardless oftheir planned specialty
The Owl
•Wherever you see the owl graphic, thatslide contains a hyperlink to additionalinformation. Click on the underlined linkon that slide
1
Diagnosis
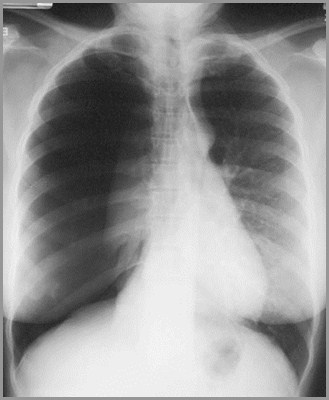
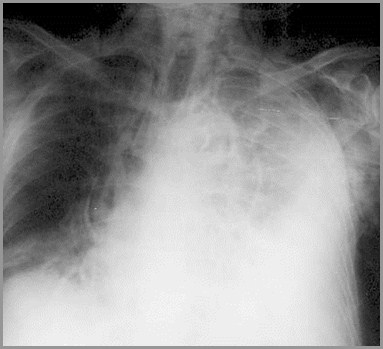
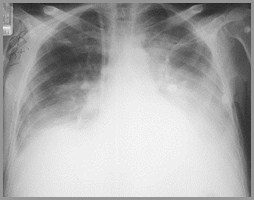
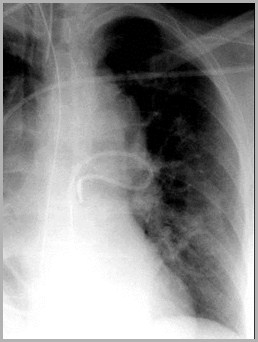
Can you tell why this patient is short of breath?
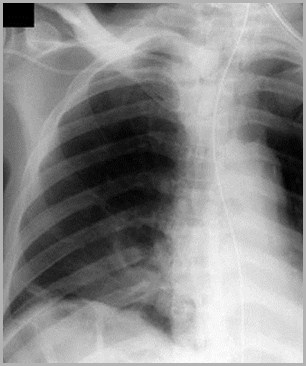
Tension pneumothorax
Complete right-sidedpneumothorax
Lung iscompressedagainstmediastinum
Shift of heartand trachea toleft
Tension pneumothorax
Pneumothorax
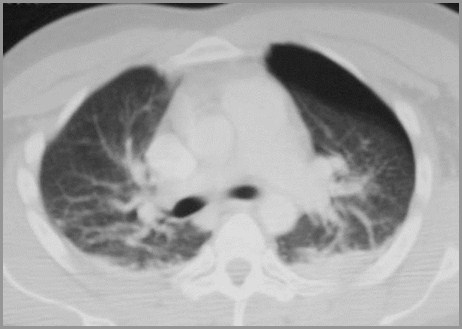
Post
Ant
With person lying ontheir back, air inpleural space rises totop and displacesnormal lung

Pneumothorax
Hot-link on this page
2
Diagnosis
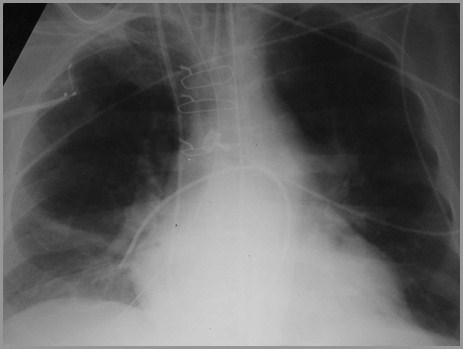
This person developed chest pain after vomiting. Why?
Pneumomediastinum from Ruptured Esophagus(Boerhaave's Syndrome)
Streaky, lineardensities dueto air in themediastinum
Streaky, lineardensities dueto air in themediastinum

Boerhaave's SyndromePneumomediastinum – CT scan
Airsurroundingesophagus inmediastinum
Extraluminalcontrast fromperforationalong leftlateral wall ofdistalesophagus
Pneumomediastinum
Hot-link on this page
3
Diagnosis
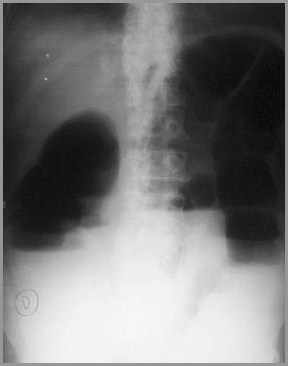
Why does this patient have abdominal pain?
Pneumoperitoneum

Air outlinesunder surface oflefthemidiaphragm
Air outlinesunder surface ofrighthemidiaphragm

Air outlines bothsides of the wallof the stomach-asign of free airin the peritonealcavity
Pneumoperitoneum
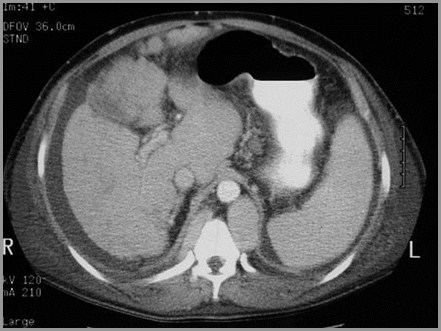
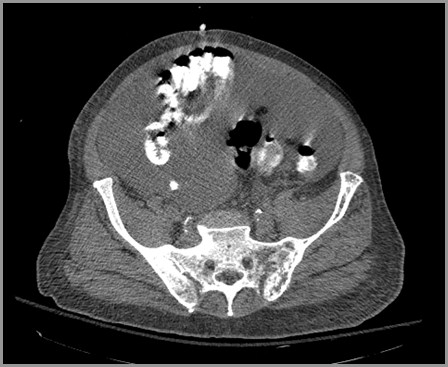
Pneumoperitoneum - CT
CT scans on 2 different people show a small and large amount of free air in theperitoneal cavity which rises to the highest point (anteriorly with the personlying on their back) and is not contained within bowel


Free air
Free air
Pneumoperitoneum
Hot-link on this page
4
Diagnosis
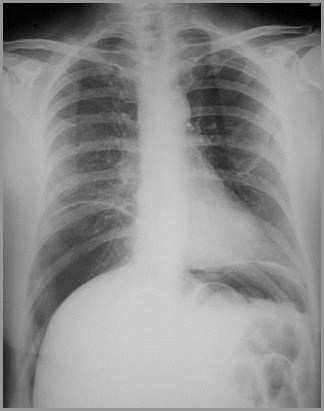
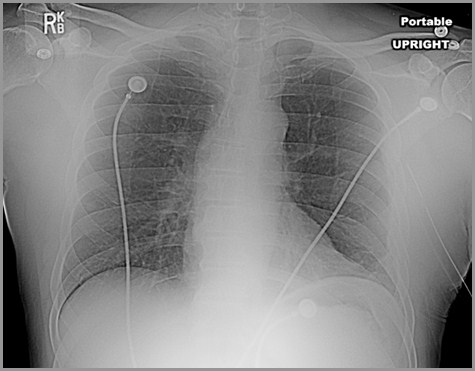
57 year-old female with shortness of breath. Why?
Bilateral Pleural Effusions


Meniscus-shaped densityat left base froma pleuraleffusion
Meniscus-shaped densityat right basefrom a pleuraleffusion
Meniscus-shaped densityat right basefrom a pleuraleffusion
Meniscus-shaped densityat left base froma pleuraleffusion
Bilateral Pleural Effusions - CT
Effect of Position - Layering

Supine
Erect
In the supine position, the fluid layers out posteriorly and produces ahaziness, especially near the bases (since the patient is actually semi-recumbent). In the erect position, the fluid falls to the bases.
Pleural Effusion
Hot-link on this page
5
Diagnosis
This patient has atrial fibrillation and a heart murmur.What’s the diagnosis?
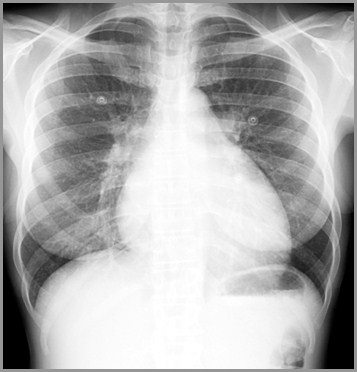
Size (notnumber) ofvessels at theapex exceedssize of vesselsat the base inthis uprightperson. This iscalled“cephalization.”Normally thevessels at thebase exceed thesize of thevessels at theapex
Pulmonary Venous Hypertension from Mitral Stenosis

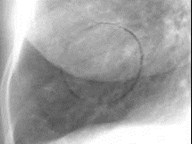
Inset of Apex of Lung
Inset of Apex of Lung
Vessels are larger atapex=cephalization

Vessels are larger atapex=cephalization
Pulmonary Interstitial Edema
Pulmonary interstitial edema with intersectingKerly A and C lines (red circle)
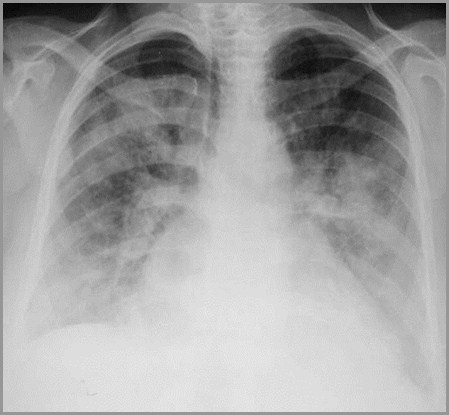
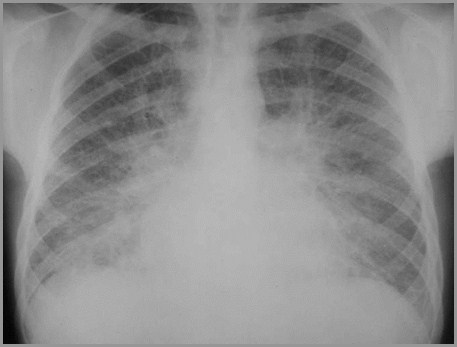
Pulmonary Alveolar Edema
Bilateral,diffuseairspacedisease moremarkedcentrallythan at theperiphery ofthe lung(“bat-wingappearance”)
Pulmonary Edema
Hot-link on this page
6
Diagnosis

63 year-old man with chest pain. Why?
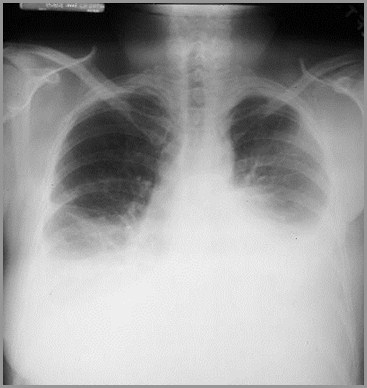
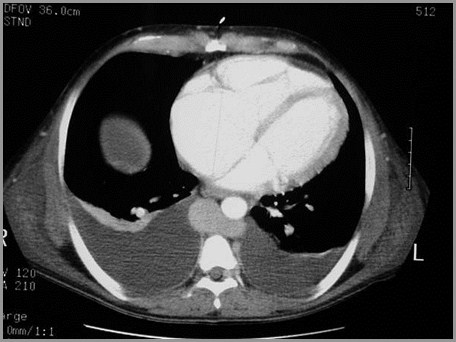
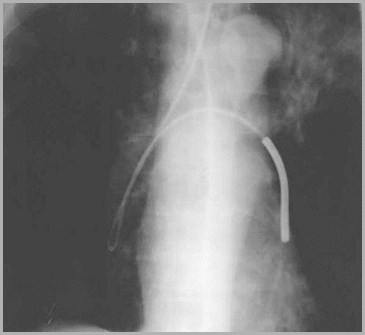
Aortic Dissection
Linear lucencyin the contrast-filleddescendingaorta is theintimal flap of anaortic dissection

Aortic Dissection
• Widenedmediastinum
• Left pleural effusion
• Chest pain
Should make you thinkof an aortic dissection

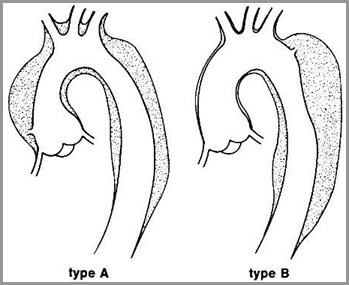
Classification of Dissecting Aneurysms
Stanford classification
• Widened mediastinum
• Left pleural effusion
• Chest pain
Aortic Dissection
Hot-link on this page
7
Diagnosis
Why did this 85 year-old haveabrupt onset of abdominal pain?
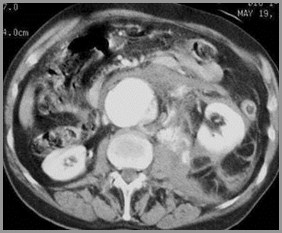
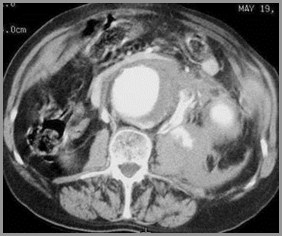
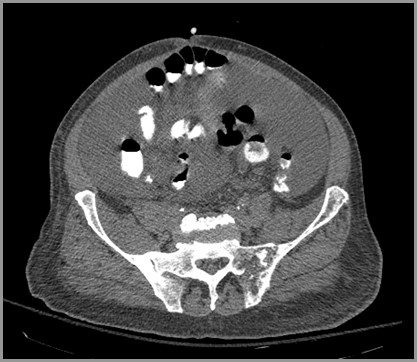
Aortic rupture
Red arrowspoint to activeextravasation ofcontrast fromthe aorta intotheretroperitoneum
Thrombusinside the lumenof the aorta
Red arrowspoint to activeextravasation ofcontrast fromthe aorta intotheretroperitoneum
Aorta
Aorta
Ruptured Aortic Aneurysm
Enlargement of abdominal aorta > 3cm
Usually 2 to atherosclerosis
Below renals, above iliacs
About 20-25% rupture
<4cm~10%; >10 cm~60%
Retroperitoneal, usually on left
Into GI tract: massive hemorrhage
Into IVC: rapid cardiac decompensation
8
Diagnosis
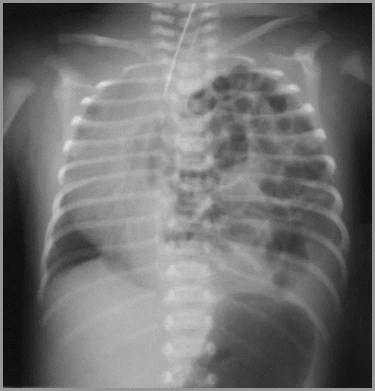
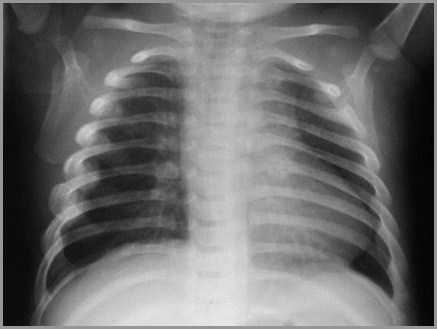
Newborn with tachypnea. Why?
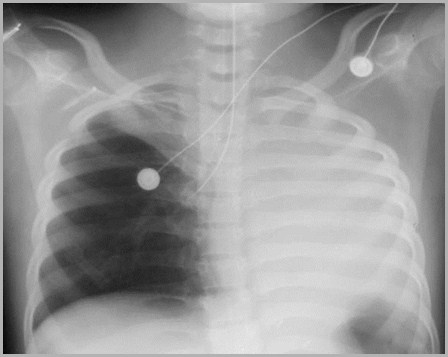
Congenital Absence of the Diaphragm
Left hemithoraxcontainsmultiplelucencies--air inthe lumen ofbowel, nowlocated in thechest
Heart andtrachea aredisplaced toright by bowel inoppositehemithorax
Congenital Absence of DiaphragmImaging Findings
Initially, hemithorax may appear opaquebecause loops are fluid-filled
Paucity of bowel loops beneath diaphragm
Once air swallowing begins, multiplelucencies contained within bowel are seen inchest
Respiratory distress may increase as intestineoccupies more of thorax
Diaphragmatic Rupture
•To learn more about congenitalabsence of the diaphragm anddiaphragmatic rupture, go to: Diseasesof the Diaphragm
Hot-link on this page
9
Diagnosis


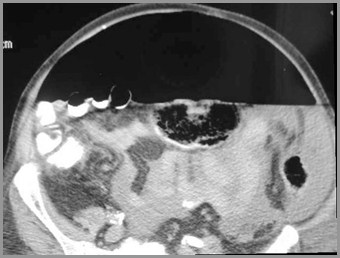
36 year-old with acute abdominal pain. Why?
Small Bowel Obstruction
Multiple air-containingand dilated loops ofsmall bowel
No gas in rectosigmoid
Multiple air-fluid levelsin smallbowel

Small Bowel Obstruction
Hot-link on this page
10
Diagnosis
83 year-old with distended abdomen.What’s the diagnosis?

Sigmoid Volvulus
Sigmoid twistsaround thispoint
Obstructed,dilated sigmoidhas a “coffee-bean” shape


Cecal Volvulus

Dilated loop inLUQ is cecumwhich hastwisted on itself

Dilated loops ofsmall bowelfrom smallbowelobstruction atileocecal valve

Sigmoid Volvulus – Barium Enema
Sigmoid twistsat this point
Dilated colonproximal tothe volvulus
Rectum
Cecal and Sigmoid volvulus
Hot-link on this page
11
Diagnosis

74 year-old with change of bowel habits. Why?

Large bowel obstruction – Sigmoid carcinoma
Dilated loops oflarge bowel withabrupt cut-off insigmoid
Barium enemashows annularconstrictingcarcinoma ofsigmoidproducingobstruction
Rectum
Dilated large bowel
Carcinoma of the Colon
Hot-link on this page
12
Diagnosis
Why does this 47 year-old haveincreasing abdominal girth?
Bowelloops aredisplacedcentrallyby asciticfluid
Ascites - CT
Ascites
Ascites islow inattenuation
R3
Massive ascites on CT
Massive ascites (redarrows) in a patientwith metastaticcarcinoma of theovary
Liver
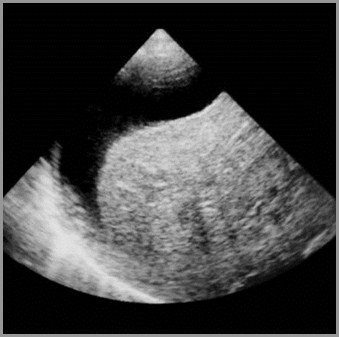
Ascites
Patient’shead
Patient’sFeet
Ascites demonstrated by ultrasound
Echo-free fluidabove liverbeneath righthemidiaphragm
13
Diagnosis
Misplaced Lines and Tubes
Tip of nasogastric tube (yellow arrow) should lieat least 10cm past the EG junction

R3
Feeding tube (green arrow) enters right lower lobe bronchus, loops onitself then crosses over to LLL bronchus (red arrow).
R3
Tip of central venous catheter coils back on itself in rightbrachiocephalic vein (red arrow).
Tip of endotracheal tube is in right mainstem bronchus (redarrow) leading to atelectasis of the right upper lobe and entireleft lung
R3

Swann-Ganz catheter enters left pulmonary artery (red arrow),then loops back on itself with tip in region of right ventricularoutflow tract (green arrow)
Tip of Swan-Ganz catheter lies too peripherally in rightdescending pulmonary artery (red arrow)
Tip of pleural drainage catheter (thoracotomy drainage tube) liescompletely outside of the left hemithorax (red arrow).
Misplaced lines and tubes
Hot-link on this page
14
Diagnosis
Child brought to Emergency Department with multiple bruises.What is the most likely diagnosis?
Healing ribfractures
Healing fractureof posterior rib(highlysuggestive ofchild abuse)
Child Abuse


Child Abuse


Metaphysealfractures likethis one arecharacteristic ofchild abuse

Metaphysealfractures likethis one arecharacteristic ofchild abuse
Fracture of tibia
Child Abuse
Bilateralsubdural orepiduralhematomas,shown here onMRI, are highlysuspicious forchild abuse
Child Abuse
Child Abuse
Hot-link on this page
15
Diagnosis
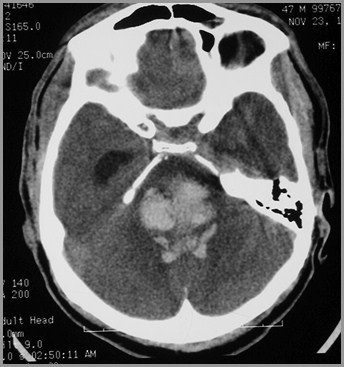
72 year-old with slurred speech. Why?
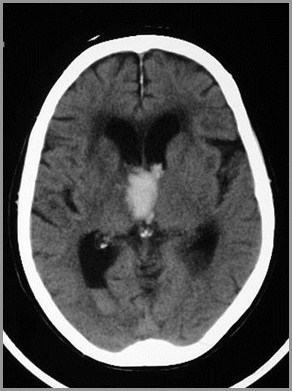
Intraparenchymal hemorrhage
Hemorrhageinto brainstemon non-contrastenhanced CT
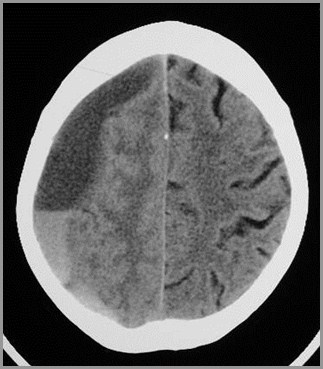
Cerebrovascular Accident with Mass effect

Shift of falx toopposite side

Largeintraparenchymalbleed
Midline shift fromhemorrhage andedema
16
Diagnosis

37 year-old hit in the head with a brick.What’s the diagnosis?
Traumatic intracranial hemorrhageEpidural Hematoma
Crescentic areaof increasedattenuation onnon contrast-enhanced CTwith convexitytoward brain ischaracteristic ofan epiduralhematoma
Traumatic intracranial hemorrhageSubdural hematoma
Crescentic lowattenuationlesion atperiphery ofbrain containinga fluid-fluid level(yellow arrow)from blood

Traumatic intracranial hemorrhageIntraparenchymal hemorrhage
Intraparenchymalhemorrhage
Acutehemorrhage onnon-contrast-enhanced CTof brain
Hemorrhage with blood in lateral ventricles
Blood settlinginto posteriorhorns of lateralventricle
Subarachnoid hemorrhage from ruptured aneurysm
R3
R3
Acute hemorrhage in the basilar cisterns (red arrows) and Sylvian fissures(green arrows) in two patients with ruptured aneurysms
17
Diagnosis
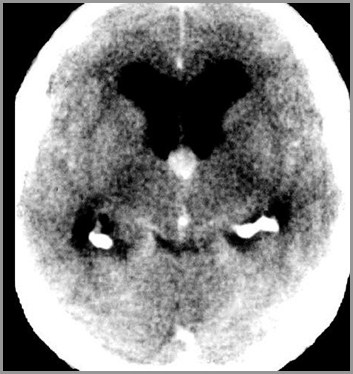
58 year-old with headache.What’s the diagnosis?
R3
Obstructive hydrocephalus caused by aColloid Cyst of 3rd ventricle
R3
Markedlyenlargedfrontal horns
Colloid Cystobstructingthirdventricle
Choroidplexus(normal)
Hydrocephalus from Choroid Plexus Papilloma

R3
Lateralventricles –anterior andposteriorhorns
Large massrepresents achoroidplexuspapilloma

Hydrocephalus from Cerebral Atrophy
Dilatedlateralventricles –anterior andposteriorhorns
Prominentsulci


Communicating (“Normal Pressure”) Hydrocephalus
Dilated thirdventricle(yellowarrow) andtemporalhorns (redarrow)

Dilated 4thventricle
18
Diagnosis
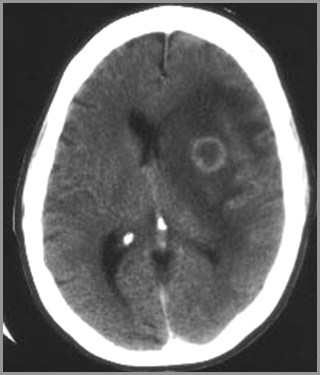
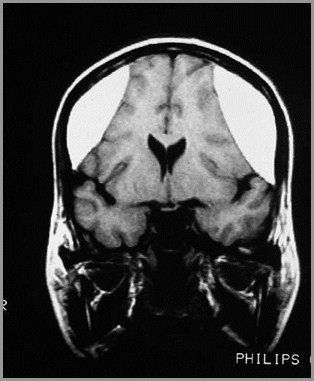
58 year-old woman with breast cancer and headache.What is the most likely diagnosis?
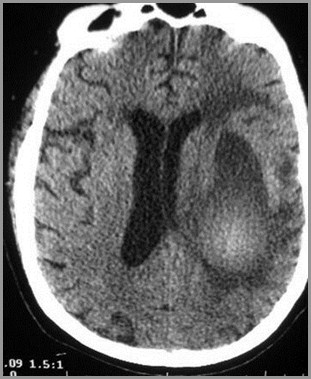
Metastatic breast carcinoma
Surroundingedema
Ring-shapedenhancinglesion withconsiderableedemasurrounding it
Shift of falxdue to masseffect of edema
19
Diagnosis


Two different people who fell injuring neck.What are the diagnoses?
A
B
Fracturethroughposteriorelements of C2
Forwarddisplacementof the body ofC2 (red arrows)
Spinolaminarwhite line of C2does not alignwith othervertebral bodies
Fracture of C2 - “Hangman’s Fracture”
A
A
A
Hangman’s Fracture
Most common fracture of C2
Most common cervical spine fracture
Hyperextension/compression fracture
Fractures through the pedicles of C2 withanterior slip of C2 on C3
Not associated with neuro deficit


Locked facets
The inferiorarticular facet ofC5 (red arrow) hasslipped forwardand lies anteriorto the superiorarticular facet ofC6 (green arrow)— a conditionknown as a“locked facet”
C5
C6
B
B
Cervical Spine Injuries
Hot-link on this page
20
Diagnosis


Two patients – one with pain in the ankle,the other with pain in the wrist
Fractures of themetaphysis (redarrow) andepiphysis (greenarrow) (Salter-Harris IV) extendinto joint
Fracture ofradial styloid(yellow arrows)extends intowrist joint
Fractures extending into joints
Fractures and Dislocations
Hot-link on this page
21
Diagnosis


27 year-old fell on elbow.What’s the diagnosis?
Posterior “fat-pad sign”indicates fluidin the joint
Fracture ofradial head
Fracture of the radial head with traumatic joint effusion
Fractures and Dislocations
Hot-link on this page
22
Diagnosis




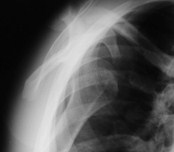

Two different patients with acute shoulder pain. Why?
1
2
Anterior Dislocation of the Shoulder
2
Humeral head(red arrow) liesinferior to thecoracoidprocess of thescapula (greenarrow)
Humeral head(red arrow) liesinferior to theglenoid fossaof the scapula(yellow arrow)
Humeral head(red arrow) liesinferior to thecoracoidprocess of thescapula (greenarrow) andanterior to theglenoid (yellowoval)
Posterior Dislocation of the Shoulder
1
Humeral head(red arrow) liesposterior tothe glenoidfossa of thescapula(yellow arrow)
Humeral head(red arrow) liesbeneath theacromionprocess of thescapula (greenarrow) andposterior toglenoid (yellowoval)
Humeral head(red arrow)assumes theshape of a“lightbulb”because it isfixed ininternalrotation
Fractures and Dislocations
Hot-link on this page
The 22 “Must-See” Diagnoses
The 22 “Must-See” Diagnoses
The 22 “Must-See” Diagnoses