
Ultrasound and CorrelativeImaging of Renal TransplantsMarch, 2012
Mindy M. Horrow, MD, FACR, FSRU, FAIUM
Director of Body Imaging
Einstein Medical Center, Philadelphia, PA
Professor of Radiology
Thomas Jefferson University
Outline
•Introduction
•Normal gray scale and Doppler evaluation
•Collections
•Infections
•Vascular Complications: Renal Artery, RenalVein, AVF, PSA
•Other: tumors, calcifications, hernias,miscellaneous
•Pitfalls and Bonus Cases
Clinical Perspective
•Most effective primary treatment of CRF
•Anticipated graft survival of 90 – 95%
–New generation immunosuppressives (cyclosporin,tacrolilmus) reduce T-cell activation, improving graftsurvival by almost eliminating acute rejection
•Demand for renal transplants greater thansupply
–Extended donor supply with older kidneys, multiplerenal arteries, etc.
★ Greater imaging challenges ★
Cosgrove D, Chan K. USQ 2008;24:77-87
Surgical Technique
•Vascular supply from end-to-sideanastomosis of donor artery and vein toexternal iliac artery and vein. If multiplearteries, usually joined with singleanastomosis to EIA
•Ureter anastomosed to superolateral wall ofurinary bladder
•En bloc transplant of a set or pediatrickidneys with caudal ends of IVC and Aortaanastomosed end-to-side to recipient's EIAand EIV, or with separate anastomoses
•Usually extraperitoneal, right side preferred
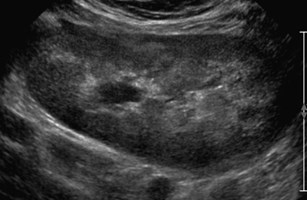
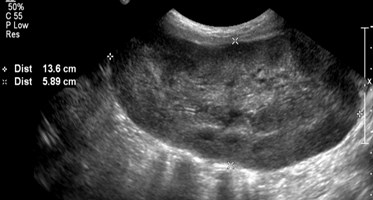
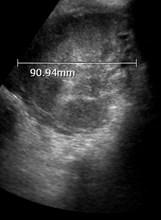
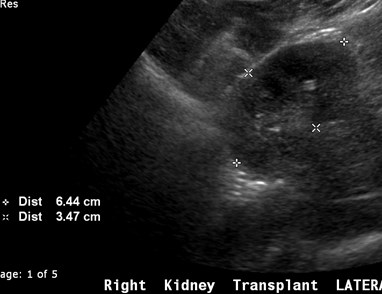
Grey Scale Evaluation
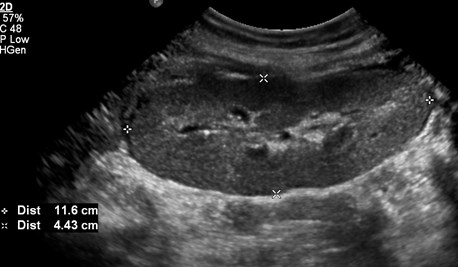
•Usually parallel to incision with hiluminferiorly and posteriorly
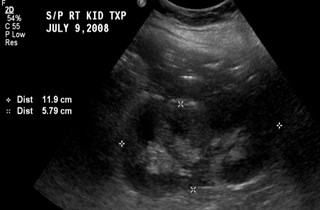
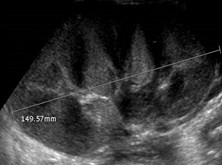
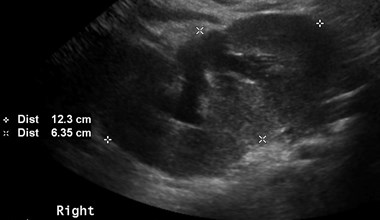
•Obtain longitudinal and transversemeasurements. Usually hypertrophies~ 15% in first 2 weeks and mayincrease by 40% in first 6 months.
Absy. Br J Radiol 1987;60:525
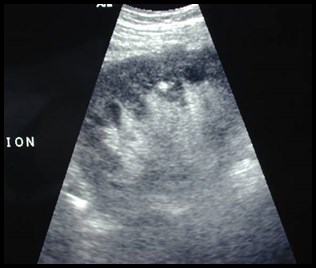
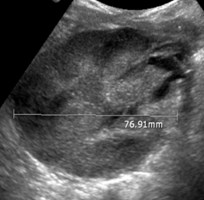
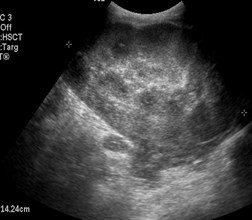
Grey Scale Evaluation
•Because kidney is more superficial,pyramids are more easily visualized,accentuating the cortico-medullarydifferentiation.
•Evaluate for any intrinsic pathology:calculi, tumors, etc.
•Collections, hydronephrosis, urothelialthickening
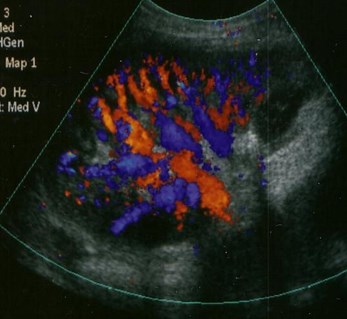
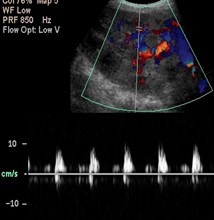
Doppler Evaluation
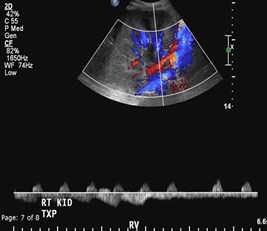
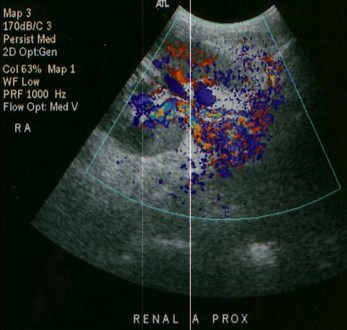
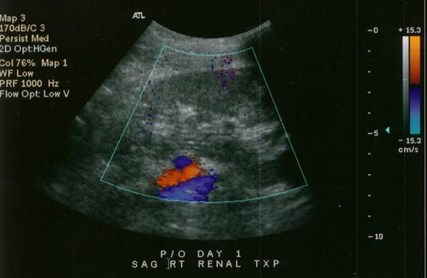
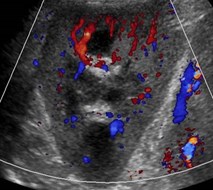
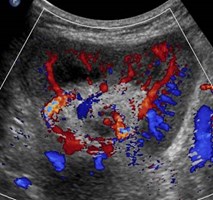
•Screen and image with color/power Doppler,looking for focal and/or diffusehypoperfusion.
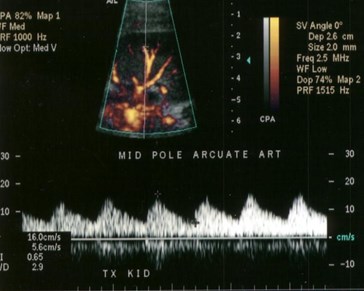
•Obtain spectral traces of arcuate orinterlobar arteries in upper, mid and lowerpoles with appropriate factors.
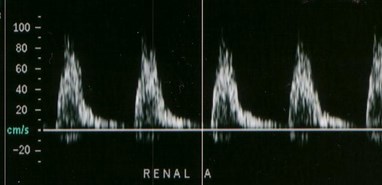
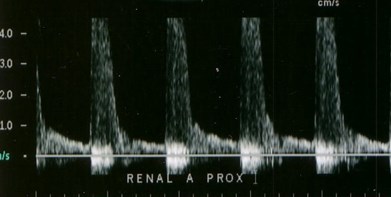
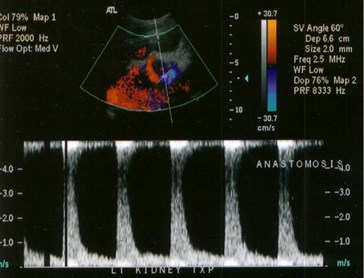
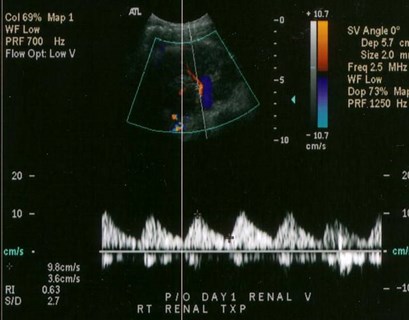
•Image and obtain spectral Doppler of mainrenal artery and vein and external iliac arteryand vein with attention to anastomoses

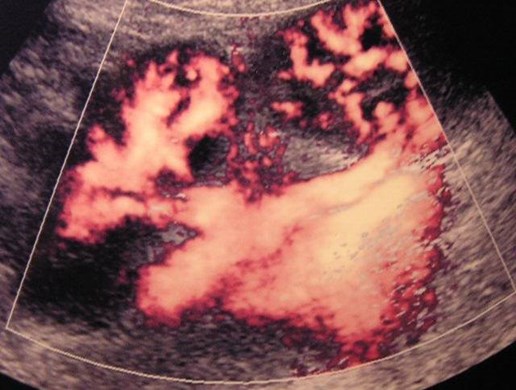
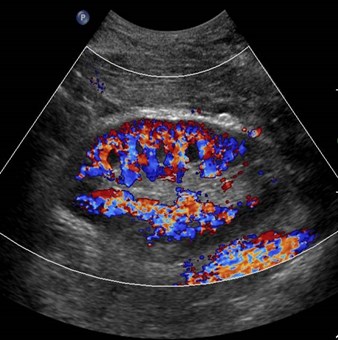
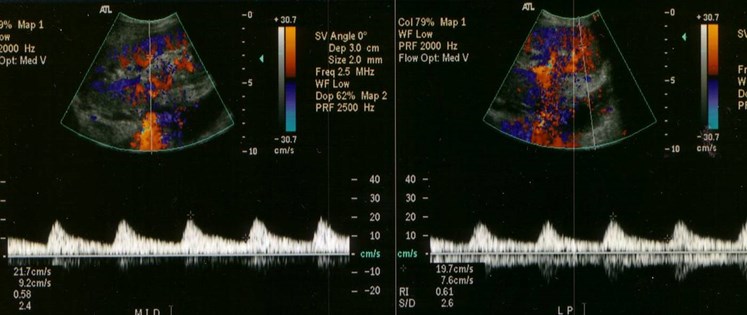
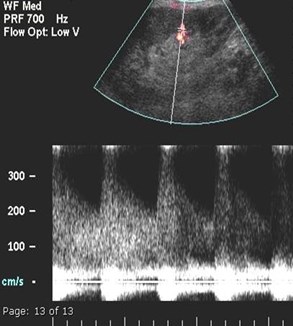
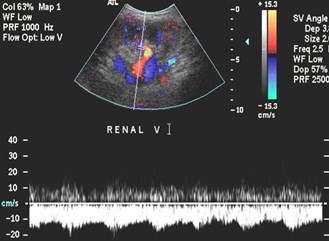
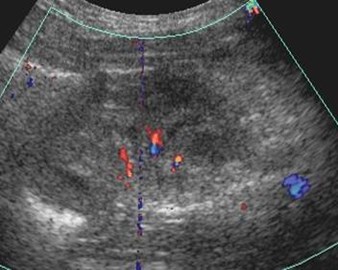
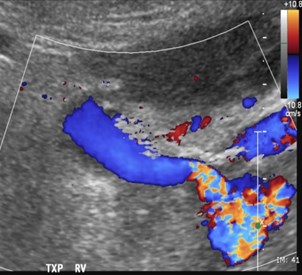
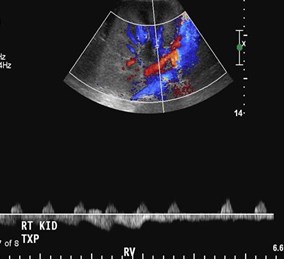
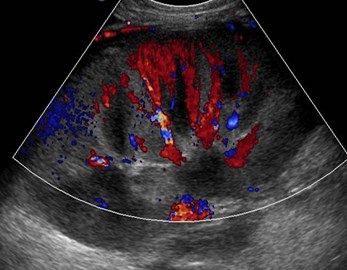
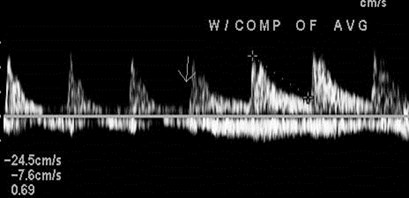
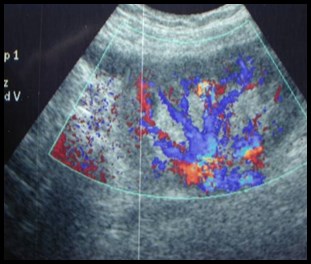
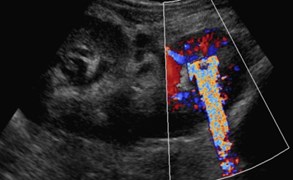
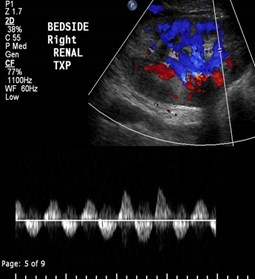
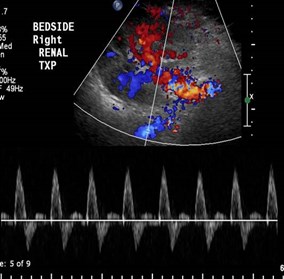
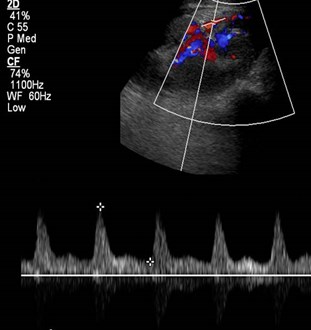
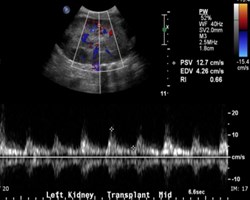
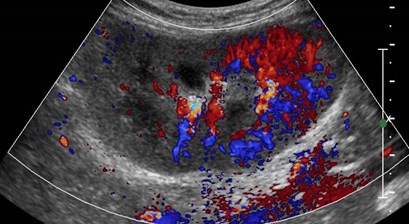
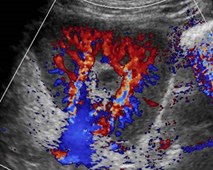
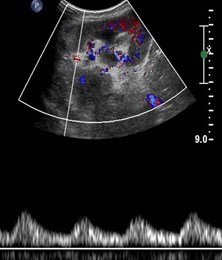
Normal color andspectral Doppler

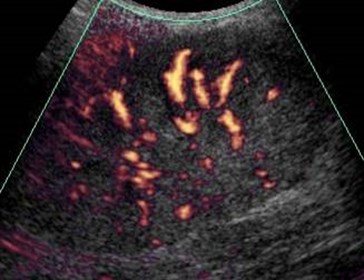
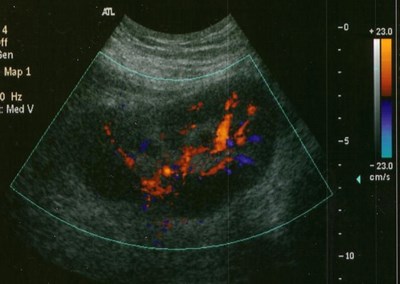
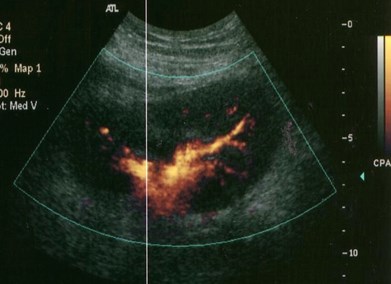
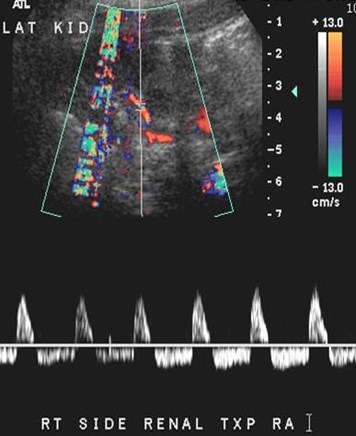
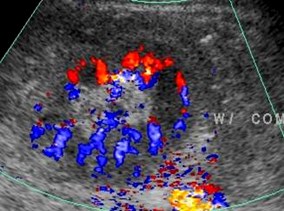
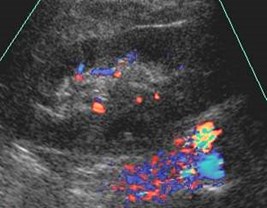
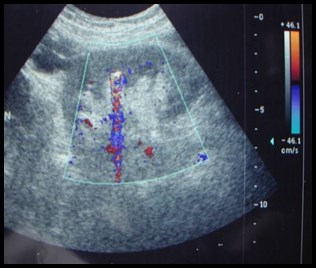
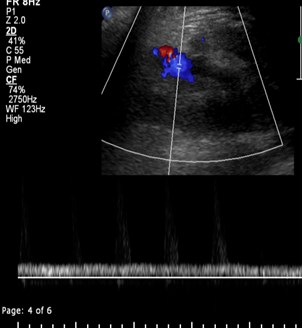
Normal power Doppler of en bloc pediatrickidney transplants
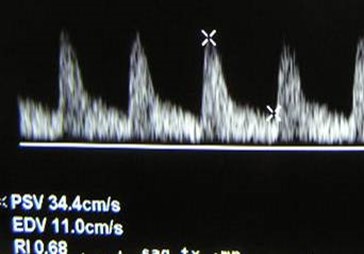
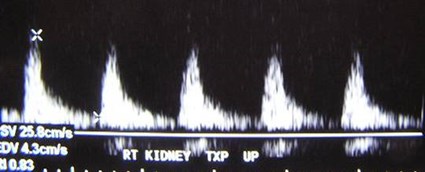
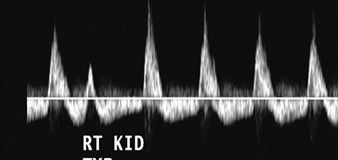
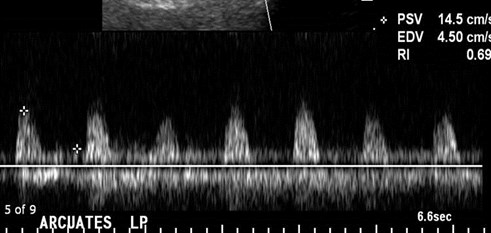
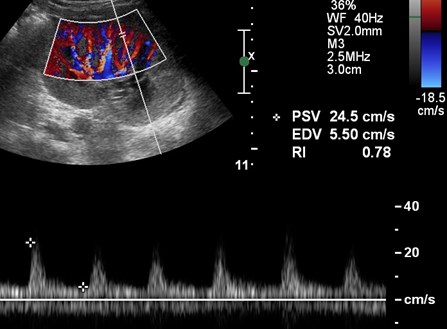
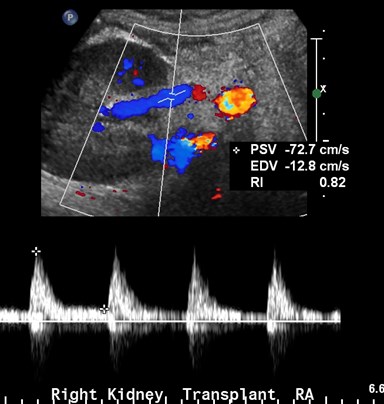
Normal Doppler Findings
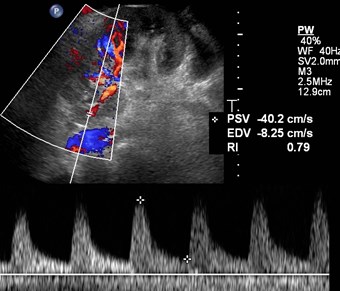
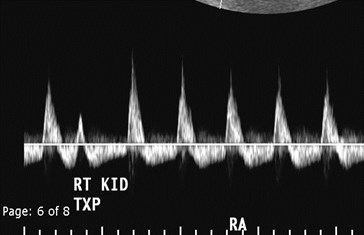
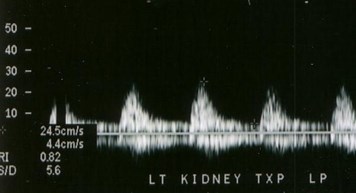
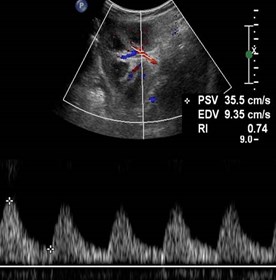
•Arteries- brisk upstroke, low resistance withnormal resistive index of 0.6 to 0.8.
–Resistive Index= (Peak systole – End Diastole) / Peak Systole
•Normal velocity main renal artery < 200cm/sec, RA/EIA velocity ration < 2
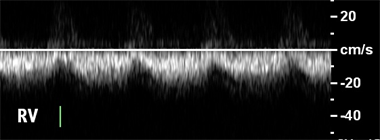
•Veins- may be monophasic with continuousflow or demonstrate some pulsatility withcardiac cycle.
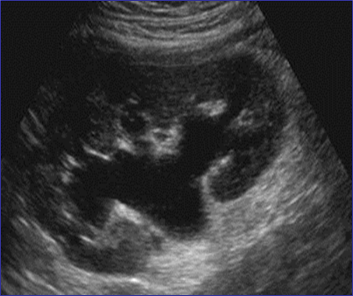
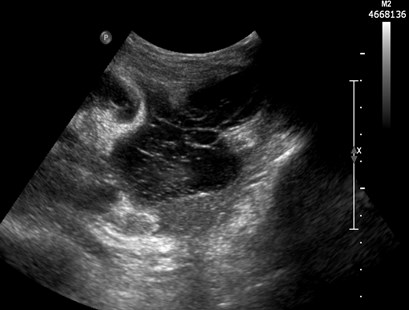
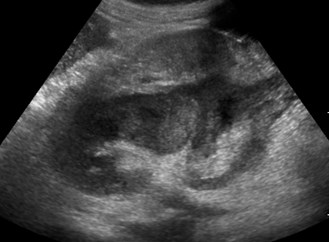
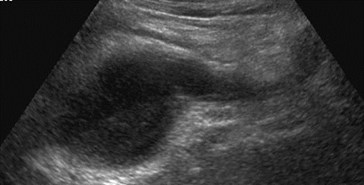
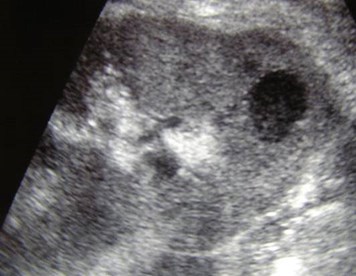
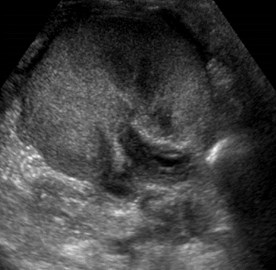
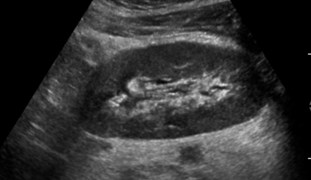
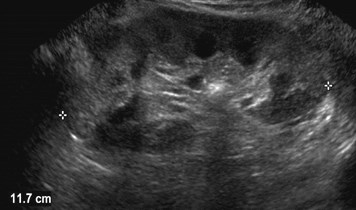
Hydronephrosis
•Obstruction is rare,though will usually beat UV junction fromstricture or intra-luminal lesion.
•Mild dilatation may be2º increased urinevolume of sole kidney,decreased ureterictone, U-V reflux


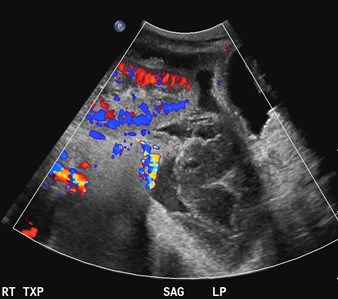
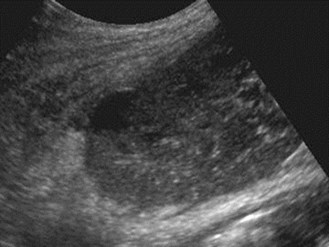
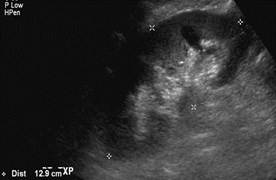
Lymphocele


Lymphocele with some pressure effect on kidney
Day One after transplant
Superficial hematoma notappreciated on US


Inferior to kidney
Hydronephrosis secondary to stenoticureter with associated urinoma

Intraperitoneal Transplant
Hemoperitoneum

Gas containing peri-renal abscess
Initial imaging
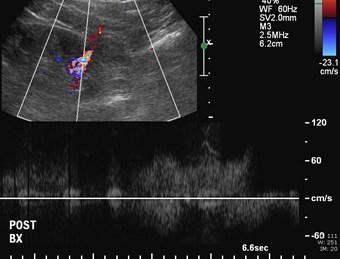
Imaging 1 day post biopsy

Subcapsular hematoma causingelevated resistive index
Fluid Collections
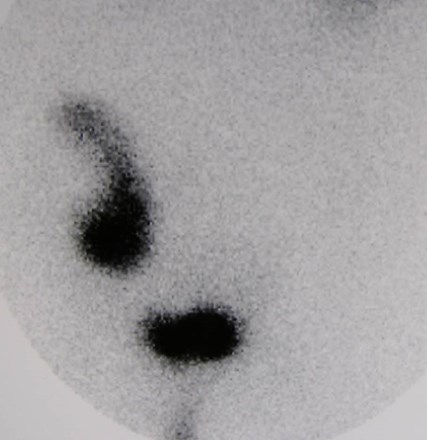
•Post- operative hematomas- appearancedepends upon chronicity.
•Urine leaks or urinomas- due to anastomoticleaks or ureteric ischemia. Appear well defined,anechoic with occasional hydronephrosis. Mayuse radionuclide imaging to confirm nature ofcollection
•Lymphoceles- occur 4 – 8 weeks after surgeryin 15%. May obstruct ureter or veins. Appearwell defined and either anechoic or with fineseptations.
Brown. Radiographics 2000;20:607
Park, etal. JUM 2007;26:615-633
Parenchymal Pathology
•Acute Tubular Necrosis
•Rejection
•Drug Nephrotoxicity
Acute Tubular Necrosis
•Occurs to some extent in all cadaverictransplants
•Most common cause of delayed graft function(need for dialysis in 2 weeks post transplant)
•Non-specific imaging features: normal orchanges in echogenicity, qualitativelydecreased color flow, RI may be normal orincreased.
Acute Tubular Necrosis, 6 days aftertransplant
Rejection
•Hyperacute- rarely imaged since itoccurs during surgery
•Acute- occurs in up to 40% in first fewweeks and is a poor long termprognostic indicator.
•Similar US and radionuclide findings
•US findings non-specific

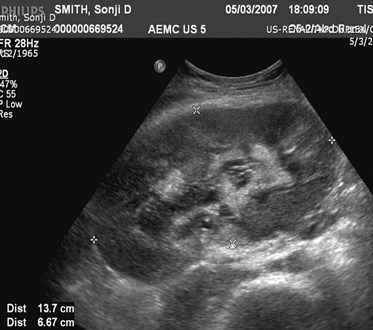
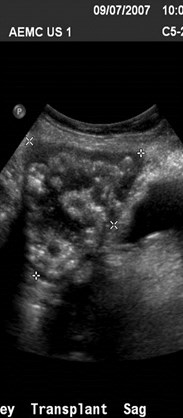
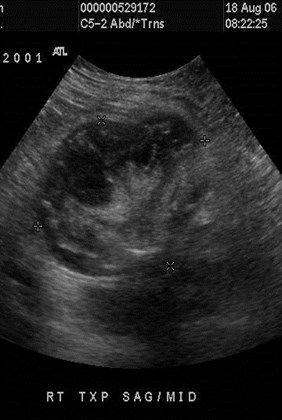
Increased size and urothelial thickening:Acute on Chronic Rejection

Patient on dialysis, anti-rejectionmedications withheld
Severely enlarged, painful kidneywith marked urothelial thickening,required nephrectomy
(has potential for rupture)

9-07
11-07
Baseline imaging Repeat because of rising creatinine
11-07
9-07
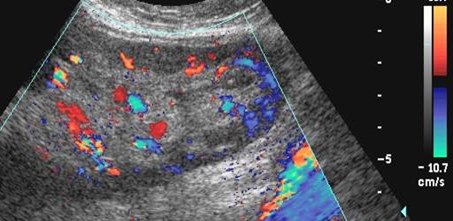
Acute Rejection: reversed diastolic flow,urothelial thickening, marked enlargement
Chronic Rejection
•Most common cause of late graft loss.
•Progressive loss of renal functionbeginning 3 months after transplant.Patients with acute rejection arepredisposed.
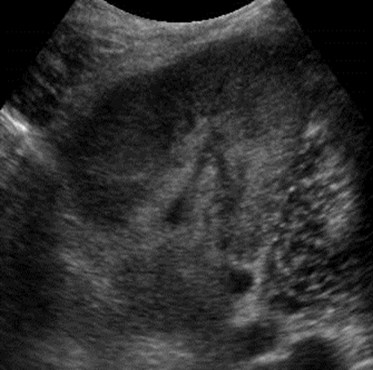
•US- Cortical thinning, mildhydronephrosis, prominent sinus fat,dystrophic calcifications, decreasedcolor, normal or increased RI.
Chronic Rejection
Chronic Rejection:progressive nephrocalcinosis
Infections
•Pyelonephritis
•Pyonephrosis
•Abscess

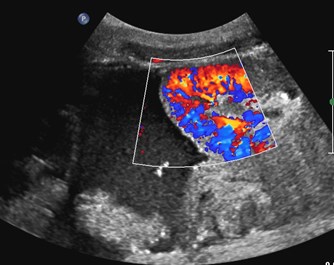
5 years after transplant with vomiting,dehydration and elevated creatinine


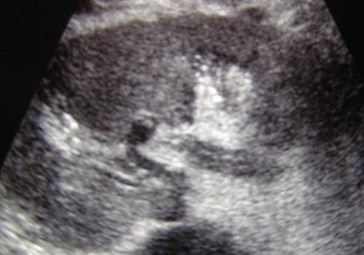
Pyelonephritis
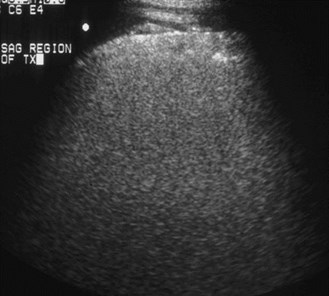
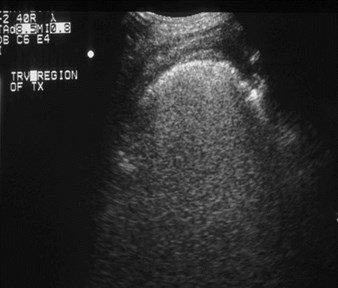
Swelling over region of one week oldtransplant with elevated creatinine


Emphysematous Pyelonephritis


Pyonephrosis


Patient with fever,imaging with 5-2MHz transducer

Imaging with 7-4 MHztransducer
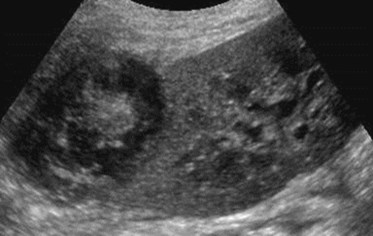
MultipleAbscesses
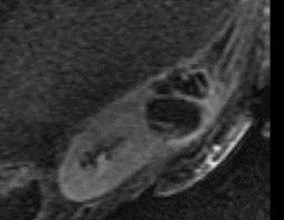
June
July
T2 with gadolinium
Renal Abscess drained percutaneously
Vascular Complications
•Renal Artery: thrombosis, stenosis, kink,pseudoaneurysm, arteriovenous fistula
•Renal Vein: thrombosis, stenosis
•Infarct
•“Steal phenomenon”


Immediatepost operativeUS
Renal Artery Thrombosis
Renal Artery Thrombosis
•Occurs in < 1% typically within first month.
•Most common cause is acute rejection withretrograde thrombosis of small to largearteries.
•Other causes: pediatric kidneys, emboli,acquired stenosis, hypotension, vascularkink, hypercoagulable state, pooranastomosis, trauma
•US: Absent arterial and venous flow inkidney and main renal artery.

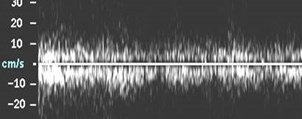
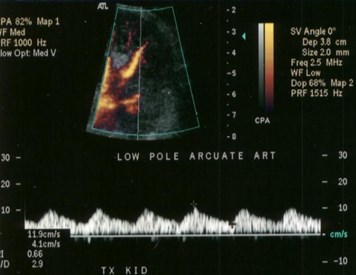
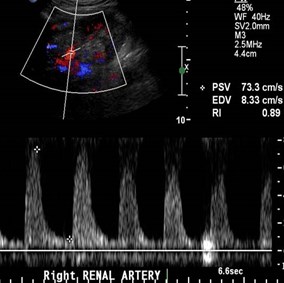
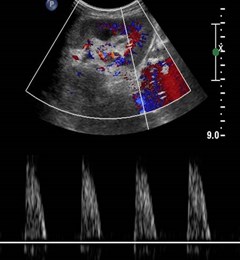
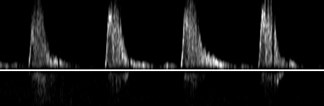
Parvus-tardus waveforms in arcuate arteries

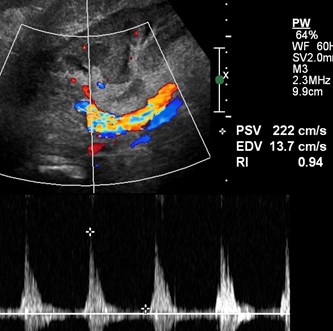
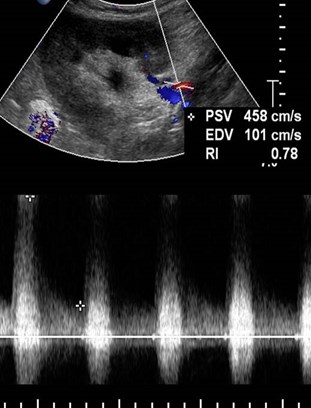
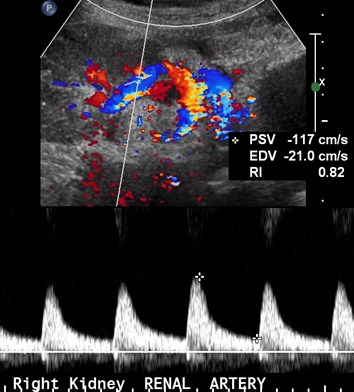
Renal Artery Stenosis
•Most common vascular complication in up to10% in first year.
•Three possible sites:
–Donor portion, typically at end-to-sideanastomosis
–Recipient portion- more uncommon, fromintraoperative clamp or intrinsic atherosclerosis
–At anastomosis- more frequent in end-to-endanastomoses
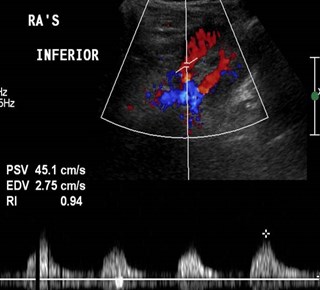
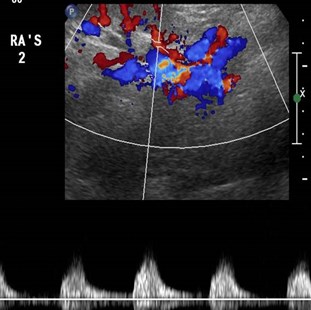
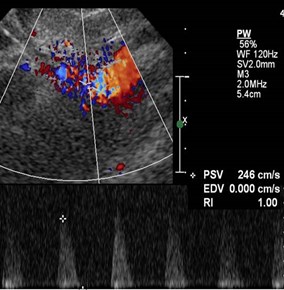
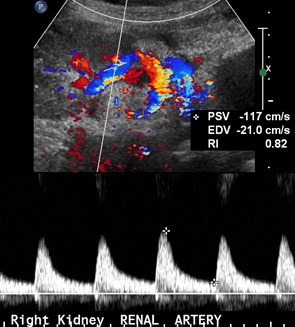
US Findings of RAS
•Parvus-tardus flow in intra-parenchymalvessels
•Use color Doppler to locate stenosis. Peaksystolic velocities > 200 cm/sec withturbulent flow.
•False positive diagnoses may occur withabrupt turn in the main renal artery.
•With chronic rejection, segmental renalartery stenoses may occur
Dodd. AJR 1991;128:1581

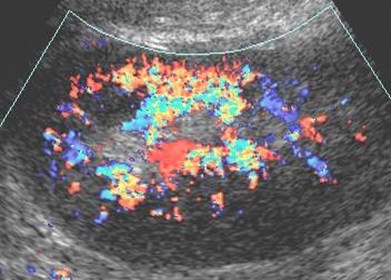
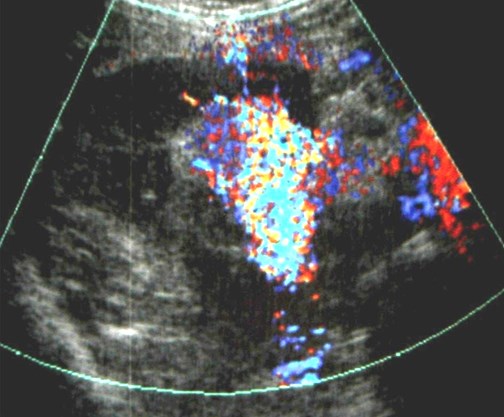
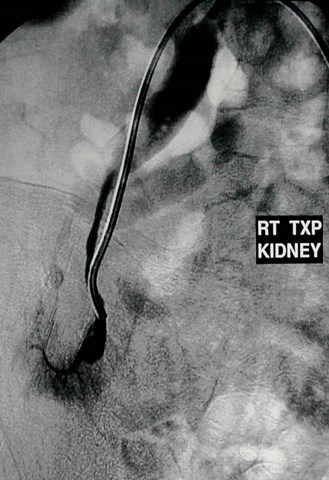
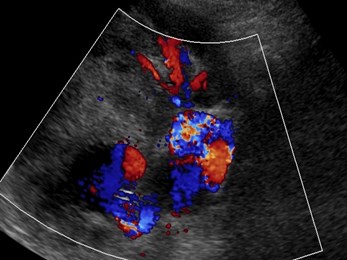
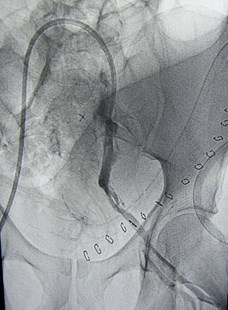
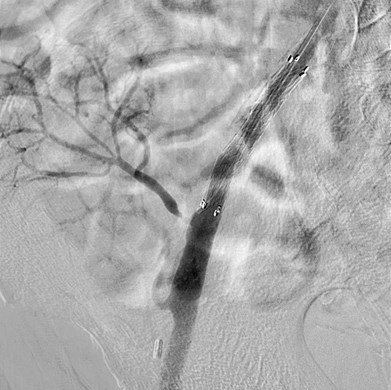
Early venous opacification impliesArteriovenous Fistula

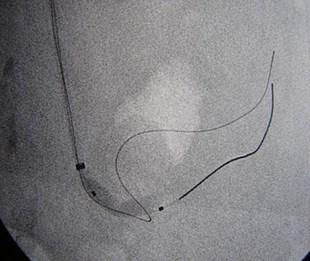

Angioplasty of stenosis reveals AVF

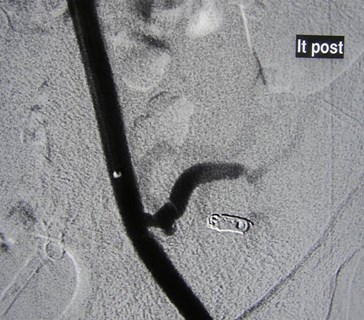
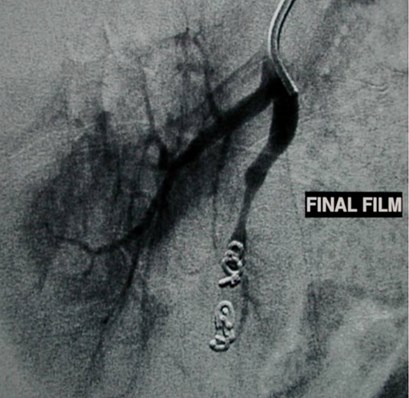
Embolization of AVF with coils
Residual renal artery stenosis
Residual stenosis,coils and small infarct
Day One afterRenal TX
Day Two


Renal Artery Kink
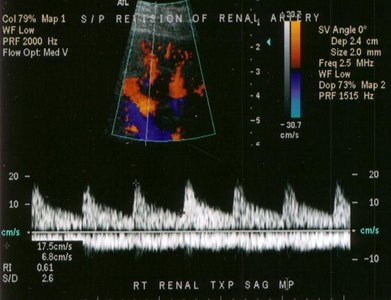
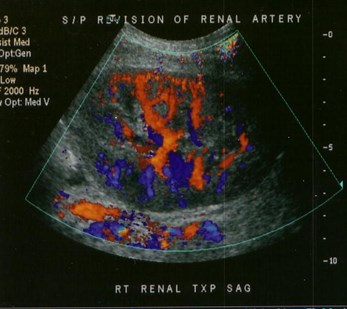
S/P revision of renal artery
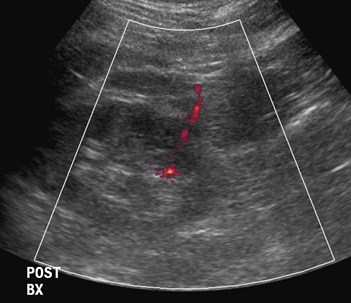

Immediately after biopsy

2 days later
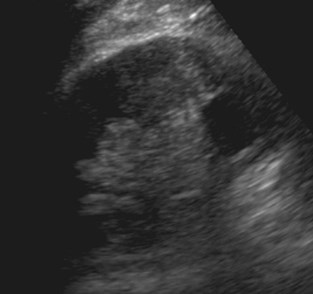
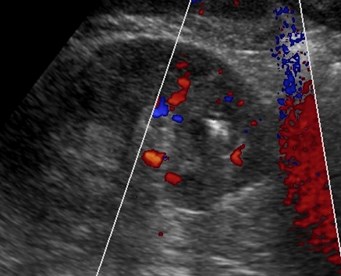
Pseudoaneurysm

Successful coil embolization
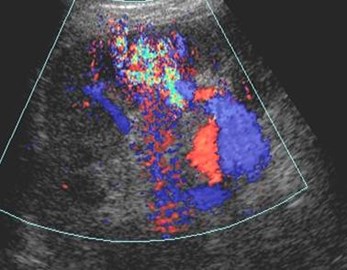
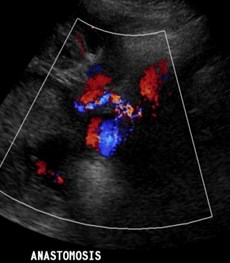
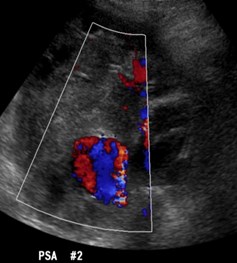
Arteriovenous fistula andPseudoaneurysm
AVF and PSA
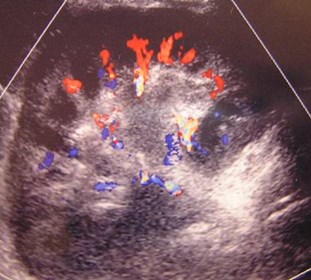
•Both are typically the result of trauma duringpercutaneous biopsy.
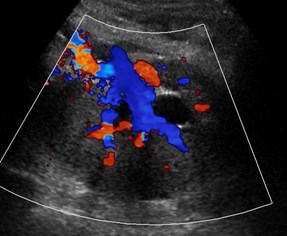
•AVF- color shows focal area of mixed colorsoccasionally with feeding vessels. AVMproduces vibrations which result in colorassigned to the perivascular tissues.
•PSA- may appear as a simple cyst on greyscale imaging but with typical swirling arterialflow on Doppler
A-V Fistula
Bacteremia


Mycotic Aneurysms require stentthrombosis and sacrifice of kidney
Renal Infarct
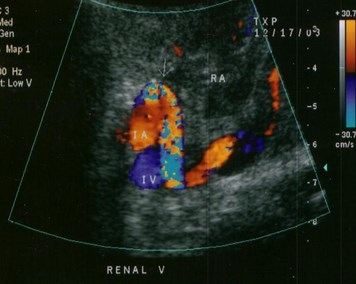
Acute Renal Vein Thrombosis

CFV w/o CFV w


Initial image #1 thrombolysis #2 thrombolysis
Renal vein thrombosis 2º stenosisof external iliac vein
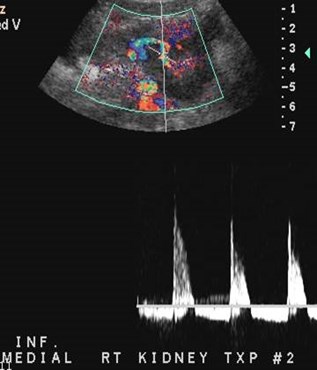
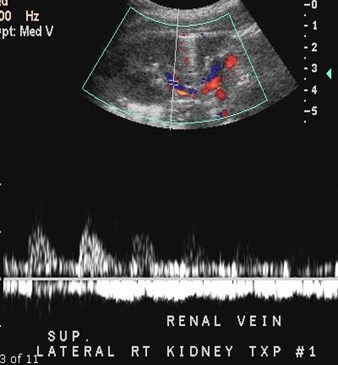
Immediate post-op imaging of en-blocpediatric kidneys
Medial kidney with renalvein thrombosis
12 hours later
Lateral kidney withrenal vein thrombosis
Venous Thrombosis
•Occurs in up to 4% transplants
•Sx: acute pain 2° swelling of kidney, oliguria infirst week
•Causes: surgical difficulties, hypovolemia,femoral/iliac vein thrombosis, compression bycollections
•US- absent venous flow, reversal of diastolic flowin artery. Kidney may be enlarged, hypoechoic.
;295
Kaveggia.AJR 1990;155:295
Reuther.Radiology 1989;170:557
Renal Vein Stenosis
•Grey Scale- normal or hypoechoic
•Color Doppler- aliasing at stenotic site
•Spectral Doppler- 3 to 4 times increasein velocity across the region indicates ahemodynamically significant stenosis.
9-18
11-15
11-30

11-30
Other images
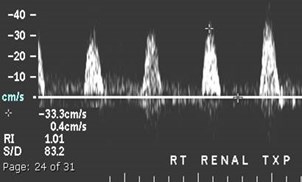
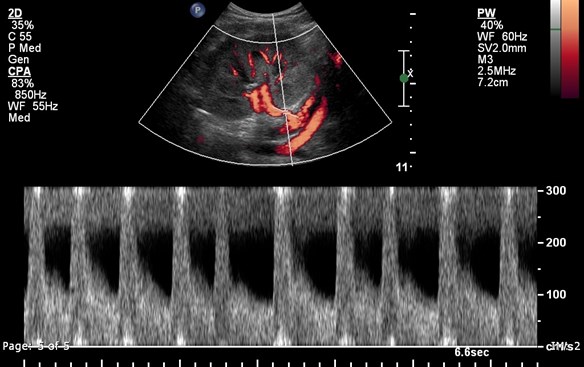
Reversed Diastolic Flow
•Though commonly ascribed to renal vein thrombosis,actually a non-specific finding
•Acute: TX < 24 hours, graft survival likely withintervention. Causes include renal vein thrombosis,hematoma, vascular kink. Since kidney lacks venouscollateral drainage, infarction occurs rapidly requiringimmediate surgery
•In more longstanding transplants causes include: ATNand rejection. These kidneys faired very poorly withhigh rate of allograft loss.
Lockhart. AJR 2008;190:650-655
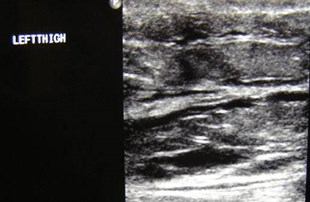
Patient with AV graft inipsilateral thigh, immediatecolor Doppler post surgery
Color Doppler duringcompression of graft
“Steal” Phenomenon
Chaudri, Horrow JUM 2006;25:939
Other
•Calcifications: calculi, medullaryand cortical nephrocalcinosis
•Tumors
•Hernia
•Miscellaneous

15 years posttransplant
Medullary nephrocalcinosisand nephrolithiasis


Early medullary nephrocalcinosis


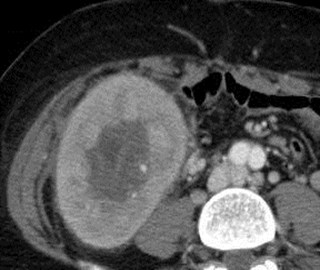
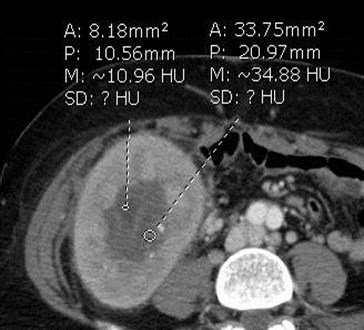
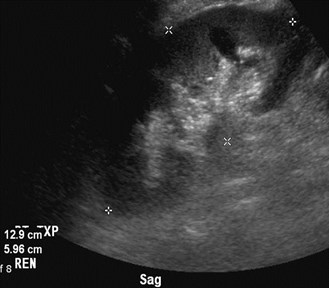
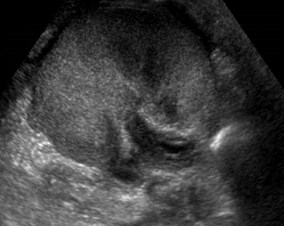
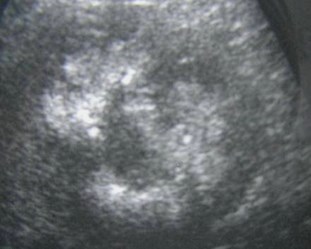
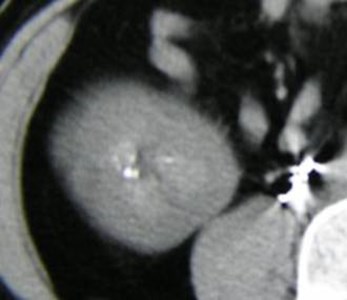
Biopsy proven renal cell carcinoma
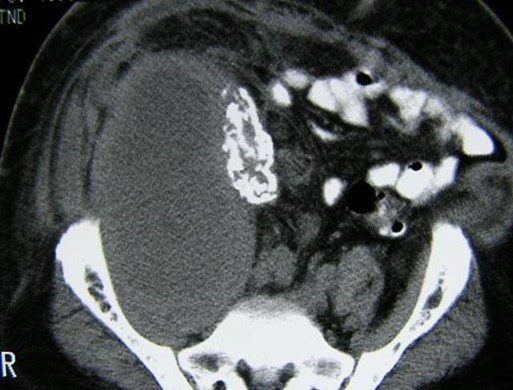
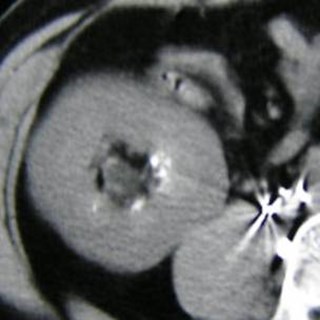
Leiomyosarcoma of failed renal transplantwith cortical nephrocalcinosis
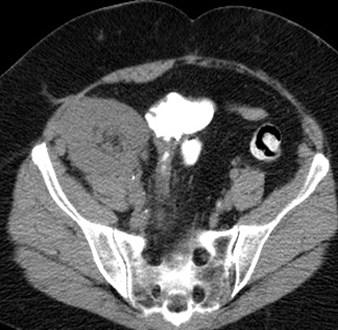
Images of left sided kidney
from double renal
transplant

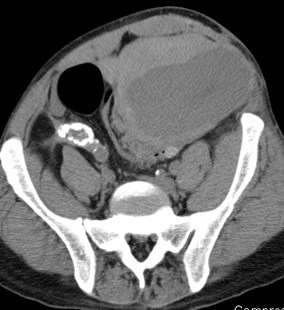
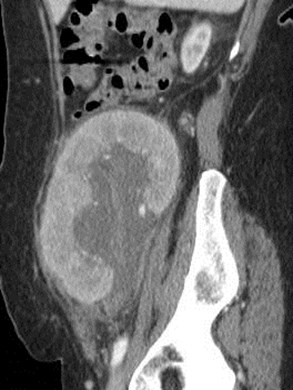
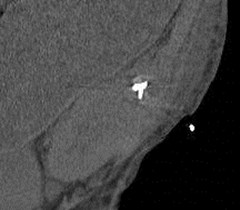
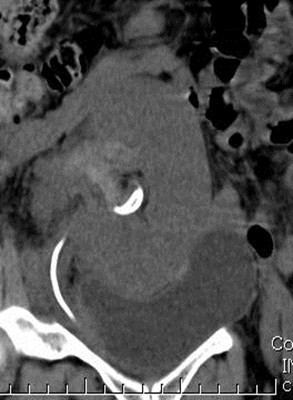
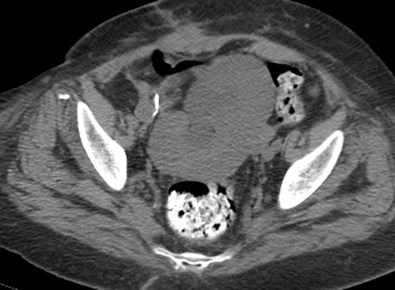
Non-contrast CT confirms left renal calculus
Also demonstrates herniation at incision
Color Doppler Twinkling Artifact
•Described in 1996 by Rahmouni as an artifact ofalternating red and blue behind certainstationary objects.Spectral Doppler of artifact generates aheterogeneous broadband signal that appears toalias.Mainly associated with nephrolithiasisSpeculation that it is generated by roughsurfaces with multiple reflectors splitting beaminto components
Rahmouni, etal Radiology 1996;199:269
5-16

8-31
Hypercalcemic secondary to hyperparathyroidismwith early calculus formation requiringparathyroidectomy and medical therapy




Calcification of urothelium

Pain over transplant
Acute appendicitis



Incisional hernia containing bowel and fluid
PITFALLSCASES
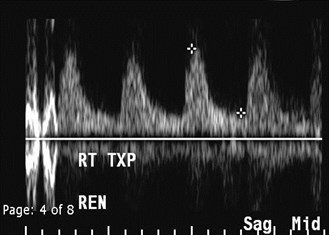
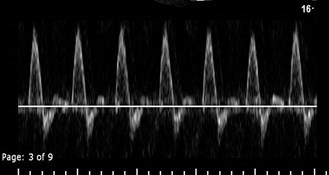
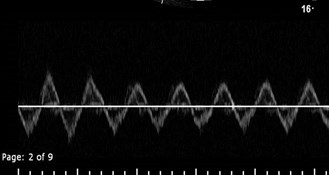
Is the resistive index measured correctly?
No- mirror image venous flow ismeasured as diastolic flow
Initial Bedside study
MRA MRV
EIA EIV
Follow Up Study
Pulsatile venous flow due to fluid overload,improves with medical therapy
Day 1
Day 2
Pain over transplant

Patient receives 2 pediatric transplants
5-2007
10-2007
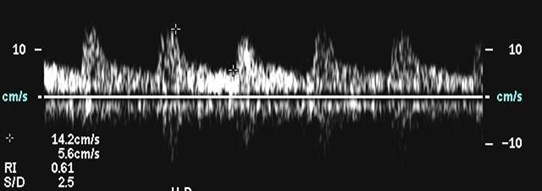
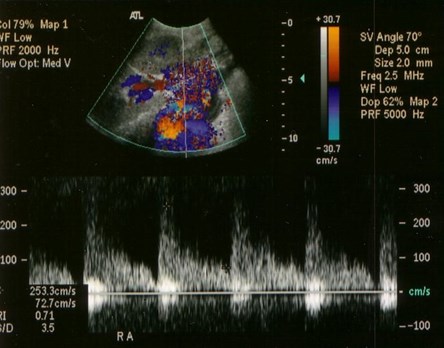
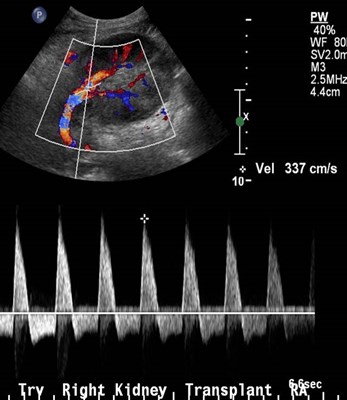
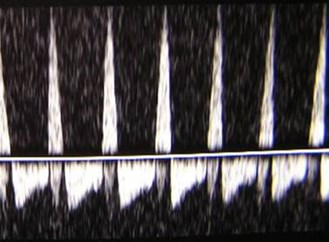
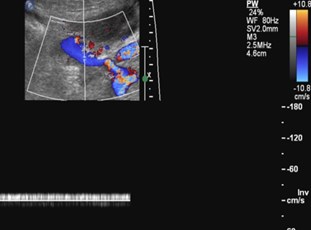
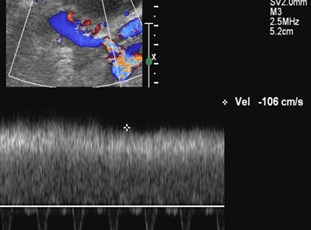
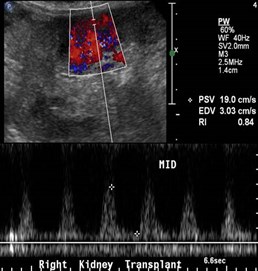
Is this renal artery stenosis?
Normal arcuate waveforms- no parvus tardus flow
High RA velocities due to high flowrate through small vessel
BONUS CASES
Early post operative imagingin renal transplant with tworenal arteries

Iliac artery stenosis, proximal totransplant
Re-imaging post stent placement
Re-imaging 2 months later with elevated creatinine
U
M
L
Lower pole Doppler
Upper pole Doppler
Interlobar
arteries
Mainarteries
Stenosis of upper pole renal artery
Origin upper pole artery
Few days later

Initial post operative study
Torsion Renal Transplant
Initial study

Pre CT Post CT
US after detorsion
The End