
Temporal Bone Fractures
Ceylan Z Cankurtaran MD
Einstein Medical Center
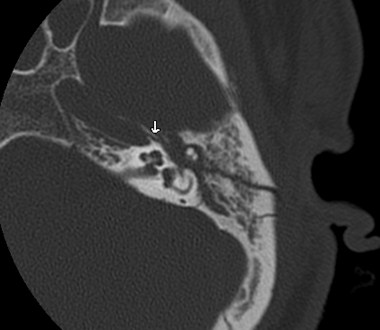
A
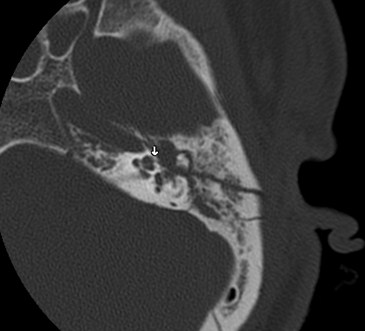
B
49 year old male status post MVA, with complex comminuted fractures of the left temporal bone.
Fractures involve the otic capsule (arrow in A) and the carotid canal (arrow in B).
T-bone Fractures
•Approximately 4% of patients treated for headtrauma have skull fractures (1)
•14–22% of patients with skull fractures havetemporal bone fractures (1)
•3 most common causes of temporal bonefractures are MVA’s (45%); falls (31%); assaults(11%) (2)
Complications (3,4)
•Facial nerve injury
•CSF leak
•Conductive hearing loss (if persistent – TM perf;ossicular discontinuity; post-traumaticcholesteatoma)
•Sensoryneural hearing loss - fracture of thelabyrinth; labyrinthine concussion; perilymphaticfistula; brainstem injury
•Other - meningocele/encephalocele, lateotogenic meningitis
Fracture Classification
•Traditional Classification :
Longitudinal vs transverse - in relation to thepetrous pyramid
•Longitudinal :
external auditory canal, TM and middle ear/ossicularinvolvement; conductive hearing loss ; FN paresis 25%
•Transverse:
may traverse the petrous apex, cross the IAC, the otic capsuleor both, involve the skull base foramina; SNHL and FN paresisreported in up to 50%

Shortcomings of TraditionalClassification (1,2,5)
•Majority of T-bone fractures are either oblique or morecomplex to be described in a planar fashion :“oblique/mixed” fractures added to terminology
•Same anatomic structures may be injured
by both types of fractures
•Poor ability of the traditional classification system
to predict complications
•Any effective classification system must be not
only descriptive but also predictive
Alternative Classification
•Alternative nomenclature proposed (1994,Kelly and Tami): “otic capsule sparing” and“otic capsule violating” in an effort to improvecorrelation with radiographic and improvesurgical planning
•Otic capsule violating fractures course thoughthe labyrinth (i.e., the cochlea, vestibule, andsemicircular canals), whereas otic capsulesparing do not
Alternative Classification
•(1997) Brodie and Thompson -
retrospective review of 820 temporal bonefractures :
incidence of FN injury correlated with otic capsuleviolating injuries
CSF fistula was twice as common in otic capsuleviolating injuries
Alternative Classification
•(1999) Dahiya et al.
5 out of 55 temporal bone fractures oticcapsule violating :
CSF leakage 4 times more likely
Severe SNHL 7 times more likely
FN paralysis twice as likely, although this did notreach significance
Petrous vs Non-petrous Fractures
•(2004) Ishman et al. analyzed 155 T- bone fractures:
“Petrous fractures” (11.6%) :
those involving the otic capsule (50%) and/or petrousapex
–x10 more likely to develop CSF leaks
–X3 more likely to develop FN injury
•better correlation with SNHL than using the“transverse” nomenclature
•No difference found between petrous and non-petrous fractures for SNHL
References
1. Piya and Aygun. Temporal Bone fractures. Emerg Radiol (2009)
16:255–265
2. Ishman and Friedland. Temporal Bone Fractures: TraditionalClassification and Clinical Relevance. (2004)Laryngoscope,114:1734–1741.
3. Brodie and Thompson.Management of Complications from 820
Temporal Bone fractures. The American Journal of Otology
(1997) 18: 188-197
4. Johnson et al. Temporal Bone Fracture: Evaluation andManagement in the Modern Era. Otolaryngol Clin N Am 41 (2008)597–618
5. Little and Kesser. Radiographic Classification of Temporal BoneFractures Clinical Predictability Using a New System. ArchOtolaryngol Head Neck Surg. (2006) 132:1300-1304.