SilicosisCoal Workers’ PneumoconiosisAsbestos-Related Disease
SilicosisCoal Workers’ PneumoconiosisAsbestos-Related Disease
Silicosis
Silicosis
SilicosisOccupational Exposure
Crystalline silica (quartz) from mining of
Coal, Graphite, Iron
Tin, Uranium, Gold
Silver, Copper
Sand blasters
Iron and steel foundry workers
Ceramic workers
Tunneling
SilicosisPathophysiology
Silica particles ingested by alveolarmacrophages
Breakdown of macrophage releasesenzymes which produce fibrogenicresponse
SilicosisNatural History
Requires 10-20 years exposure before x-ray appearance
Radiographs frequently overestimatedegree of symptoms early
Silicosis has a progressive naturedespite cessation of dust exposure
SilicosisX-ray-1
Multiple small rounded opacities
Usually in upper lobes
May have ground glass appearance
May occasionally calcify centrally (20%)
SilicosisX-ray-2
Lymph node enlargement common
Eggshell calcification of hilar nodes (5%)
DDx: Sarcoidosis
Large opacities are conglomerations ofsmall opacities
Complicated SilicosisProgressive Massive Fibrosis (PMF)
Massive fibrosis and conglomerate massformation in upper lobes with scarringand retraction of hila upwards
Progressive Massive Fibrosis (PMF) maycavitate from tuberculosis or ischemicnecrosis
Compensatory emphysema in lower lungfields
Caplan’s Syndrome
Consists of large necrobiotic nodulessuperimposed on silicosis
More common with CWP
SilicosisComplications
Predisposes to TB
Exhibits “limited” evidence forcarcinogenesis in humans
Coal Workers’
Pneumoconiosis
Coal Workers’
Pneumoconiosis
Coal Workers’ Pneumoconiosis(CWP)
Originally silica was erroneously thoughtto cause CWP
Actually due to inhalation of pure carbon
Still referred to as anthrasilicosis oranthracosis although most coal in USA isbituminous
No progression in absence of exposure
CWPNatural History
Rounded opacities of CWP, foundpredominantly in the upper lobes, do notprogress in absence of more coal dust
Coal Worker’s PneumoconiosisClassification
Classification is by the InternationalLabor Organization’s (ILO’s) 1980classification (p,q,r, etc.)
Direct correlation between amount ofcoal dust contained in lungs andprofusion category
Simple:small nodulesComplicated: larger nodules or masses
Coal Worker’s PneumoconiosisPathophysiology
Coal dust is deposited in alveolarmacrophages
Migrate to, and leave coal dust depositsaround, respiratory bronchioles
Fibrous reaction occurs
Coal Workers’ PneumoconiosisX-ray
Small, rounded opacities
Upper lobe distribution
Associated with chronic bronchitis andcor pulmonale
Coal Worker’s PneumoconiosisPMF
Most often, nodules have irregularborders with scar emphysema
Formed by fusion of groups of smallernodules
High ash content in the lungs
Nodules with regular borders andwithout scar emphysema
Arise from the enlargement of single nodule
High carbon content and little ash in lung
Complicated CWP
Large masses in
Upper lobes or
Superior segments of lower lobes
Unlike silicosis, large upper lobelesions of CWP are single (rather thanconglomerate) black masses with liquidcore, not fibrous tissue core
Masses may undergo cavitation eitherfrom TB or ischemia
Asbestos-RelatedDisease
Asbestos-RelatedDisease
Asbestos ExposureGeneral
Salts of salicic acid
90% of asbestos in USA is whiteasbestos (chrysotile)
Occurs in
Automotive workers-brake linings
Shipfitters
Construction workers
Asbestos-Related DiseaseTypes of Fibers
Chrysotile (white asbestos)–benign
Crocidolite (blue/black asbestos) inSouth Africa/Australia–malignant
Crocidolite-small fibers-associated withmost pleural disease
Asbestos-Related DiseasePathophysiology
Asbestos particles invoke a hemorrhagicresponse in lung
Fibers then coated with a ferritin-likematerial resulting in ferruginous bodies
Damage to respiratory bronchioles andalveoli
Asbestos-Related DiseaseTypes of
Asbestos-related Pleural Disease
Asbestosis
Asbestos-related Malignancies
Asbestos-Related Pleural Disease
Pleural plaques
Diffuse pleural thickening
Pleural calcification
Pleural Effusion
Asbestos-Related Pleural DiseaseIncidence of Pleural Disease
Almost all have some pleural involvement
Pleural plaque65%
Diffuse pleural thickening17%
Calcification50%
Effusion21%
Pleural involvement without parenchymaldisease is common
Asbestos-Related Pleural DiseasePleural Plaques-1
Affects submesothelial layer of parietalpleura
Bilateral, mid-lung zone
Between 7th and 10th ribs
Diaphragmatic pleura
Spares apices
Asbestos-Related Pleural DiseasePleural Plaques-2
Plaques don’t usually calcify
Plaques alone are not associated withmalignancy
Appear either in “profile” or “en face”
Asbestos-Related Pleural DiseaseDiffuse Pleural Thickening-1
Diffuse thickening of parietal pleura
Involves diaphragmatic pleura, extends uplateral chest wall
Commonly obliterates costophrenic angles
Spares apices of lungs
DDX from TB
Asbestos-Related Pleural DiseaseDiffuse Pleural Thickening-2
Frequently the sequela of benign pleuraleffusion
Associated with rounded atelectasis
Asbestos-Related Pleural DiseasePleural Calcification
Pleural calcification occurs in about 50%with asbestos-related disease
Especially diaphragmatic pleura
Dense calcifications paralleling diaphragm-Pathognomonic
DDx: Talc exposure, hemothorax, old TBempyema (unilateral)
Asbestos-Related Pleural DiseasePleural Effusion
Effusion alone may occur early in disease(first 20 years) in about 3% of cases
Exudative
May be associated with chest pain
Involves visceral pleura as well
Does not mean mesothelioma
May be associated with rounded atelectasis
AsbestosisGeneral
Reserved for parenchymal lung disease
Fibrosis begins around bronchi andprogresses outward
Asbestosis
Interstitial lung disease
Rounded atelectasis
AsbestosisLocation
More common in lower lungs
More common subpleural
AsbestosisX-ray
Opacities are small and irregularly shaped
Not rounded as in silicosis
Prominent septal lines around 2° lobules
Cardiac silhouette may become shaggy
Hilar lymph nodes rarely affected
DDx from silicosis
AsbestosisHRCT
Multiple subpleural dot-likenodularities=subpleural lines
Fibrous bands
Subpleural pulmonary arcades
Honeycombing
Thickened interlobular lines
Ground-glass appearance
Asbestos-Related DiseaseRounded Atelectasis
Form of peripheral lobar collapse
Associated with pleural disease
Resembles mass
Usually at lung base
“Comet tail” appearance back to hilum
Asbestos-Related Malignancies
Bronchogenic carcinoma
Mesothelioma
Benign
Malignant
Carcinoma of the larynx or stomach
Asbestos-Related DiseaseLung Cancer
Either squamous cell oradenocarcinoma
Bronchogenic ca is almost alwaysassociated with cigarette smoking
90x more common in smokers, 5x morecommon in non-smokers
Frequently at lung base
Associated with increased risk ofstomach cancer
AsbestosisMesotheliomas-1
Benign mesotheliomas not related toasbestos exposure
Asbestos exposure found in 80% ofmalignant mesotheliomas
But other x-ray changes ofasbestosis found in only 30% ofpatients with mesothelioma
AsbestosisMesotheliomas-2
No relation between mesothelioma andsmoking
Most often due to crocidolite particles
Most often present as unilateral pleuraleffusions
During course of disease, pleural effusiondevelops in almost all patients withmesothelioma
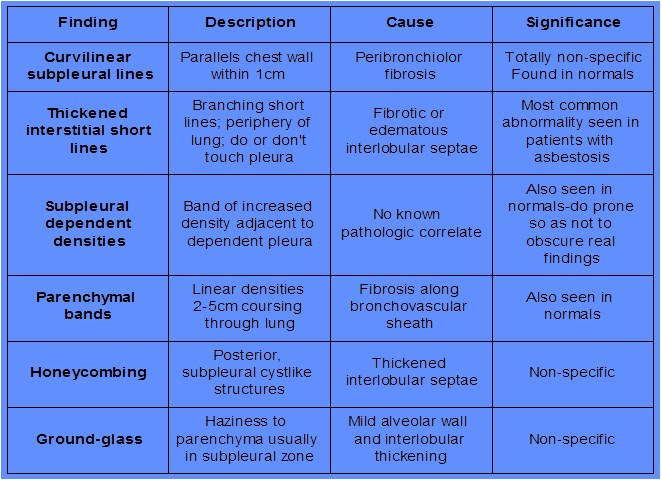
Asbestos-Related DiseaseHRCT Findings
Curvilinear subpleural lines
Thickened interstitial short lines
Subpleural dependent densities
Parenchymal bands
Honeycombing
Ground-glass opacification