
Embolic Disease
© William Herring, MD, FACR
Embolic Diseases
Thromboembolic Disease
Septic Emboli
Fat Embolism
Amniotic Fluid Embolism
Metallic Mercury Embolism
Thromboembolic Disease
Thromboembolic DiseaseGeneral-1
Only 1/3 of pts. with fatal PE havesymptomatic DVT
Misdiagnosed more than half the time
DVT suspected clinically <30%
Most emboli do not produce infarction
Thromboembolic DiseaseSites
Mostly lower lobes
Greater blood supply
Usually multiple (62%)
Bilateral half the time
Thromboembolic DiseaseClinical
Dyspnea (86%)
Pleuritic chest pain (72%)
Cough (70%)
Apprehension (59%)
Hemoptysis (34%)
Thromboembolic DiseaseImaging-1
Normal chest x-ray
Westermark's sign
Abrupt cutoff and increased caliber ofdescending branch of PA
“Knuckle” sign
Westermark’s Sign-Left LungNote the number of vessels in each lung

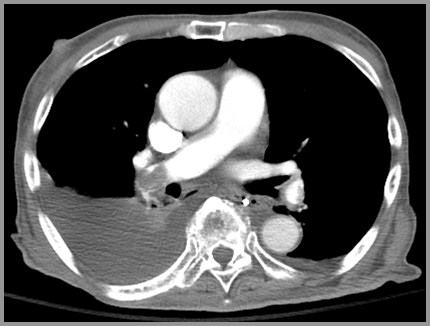
Westermark’s Sign-CTLarge left pulmonary embolus (red arrow) causesa paucity of blood vessels in left lung

Thromboembolic DiseaseImaging-2
Elevation of hemidiaphragm
Pleural effusion
Discoid atelectasis
Infiltrate
Usually basal and abutting pleural surface
Right pleural effusion-Right PE
Embolism without Infarction
Most PEs (90%)
Frequently normal chest x-ray
SSA
Pleural effusion
Westermark’s sign
“Knuckle” sign
Elevated hemidiaphragm
Embolism with Infarction
Consolidation
Cavitation
Pleural effusion (bloody in 65%)
SSA
No air bronchograms
“Melting” sign of healing
Heals with linear scar
Septic Emboli
Septic EmboliCauses-1
Two major sources
Tricuspid endocarditis
Septic thrombophlebitis
Septic EmboliCauses-2
Predisposing condition almost alwayspresent
Drug addiction
Alcoholism
Immunologic deficiencies
Congenital heart disease (shunts)
Septic EmboliImaging
Multiple solid nodules, or
Multiple thin-walled cavities
Hilar and mediastinal adenopathy may bepresent
Rapid resolution with treatment
Multiple Cavitating Septic Emboli

Fat Embolism
Fat EmbolismGeneral-1
Nearly all result from trauma
Usually leg fractures
Pathologically, fat embolism isvery common
As high as 97% after injury
Fat EmbolismGeneral-2
Carried via bloodstream as neutraltriglycerides and converted by pulmonarylipase to unsaturated fatty acids
Most common in
Young people in MVAs with leg fractures
Older people with hip fractures
Post-arthroplasty
Fat EmbolismClinical
Resp: Dyspnea, cough, hemoptysis
CNS: Confusion, restlessness, delirium,stupor
Skin: Petechiae or rash
Blood: Hypocalcemia
Calcium bound by free fatty acids
Urine: Fat in the urine
Lipiduria
Fat EmbolismImaging
Chest x-ray usually normal
Takes 1– 3 days following trauma for fullpicture to develop
DDX from lung contusion
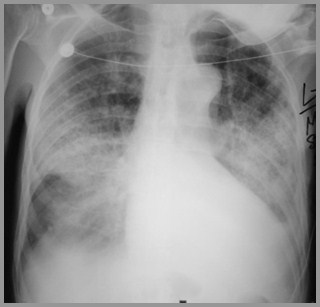
Typical appearance is pulmonary edema-like, sometimes affecting periphery orbases more than CHF does
Fat Embolism from Femur Fracture

Amniotic Fluid Embolism
Amniotic Fluid EmbolismGeneral-1
Develops only if fetal products (skin andmeconium) enter maternal blood stream
Onset is immediate
Amniotic Fluid Embolism General-2
Particles are filtered out in pulmonaryvascular bed and produce
Pulmonary arterial hypertension
Shock
Pulmonary edema
Hypoxemia
May produce rapidly fatal anaphylacticreaction or DIC
Amniotic Fluid EmbolismPredisposing Conditions
Predisposing conditions include
Multiparity
Intrauterine fetal death
Older age of the mother
Difficult or prolonged labor
Amniotic Fluid EmbolismImaging
Pulmonary edema indistinguishable fromCHF
DDX: massive pulmonary hemorrhage andMendelsohn’s syndrome
Oil Embolism
Oil EmbolismGeneral
Occurs 100% of the time followinglymphangiography
Most who demonstrate it on x-ray havelymphatic obstruction
Oil EmbolismImaging
Manifests as very fine granular, thenreticular interstitial pattern
Rarely produces symptoms
Metallic Mercury Embolism
Metallic Mercury EmbolismGeneral
May be introduced by
Drug abusers
Attempted suicide
For “Muscle quickness”
Produces mild inflammatory reaction
Excretion is via kidney
Metallic Mercury EmbolismImaging
Characteristic appearance in lungs ofdiffuse metal density
Goes to dependent portion of lung at timeof injection
Metallic Mercury Embolism

The End