
PulmonaryTuberculosis
© William Herring, MD, FACR
PrimaryPulmonaryTuberculosis
1° Pulmonary Tuberculosis
Patterns
Pneumonia
Adenopathy
Atelectasis
Pleural effusion
Primary TuberculosisPneumonia
Upper lobes affected slightly more than lower
Pneumonia common
Cavitation is rare
Lobar pneumonia almost always associated withlymphadenopathy
Infiltrate + ipsilateral adenopathy–think TB
Primary TuberculosisAdenopathy
Unilateral hilar and/or paratracheal
Usually right-sided
Rarely bilateral
Differentiates 1° from 2°—does notoccur in postprimary TB
Adenopathy much more common inchildren

Unilateral Hilar and MediastinalAdenopathy from Primary TB
Primary TuberculosisAtelectasis
Classically affects anterior segmentsof upper lobes, or
Medial segment of the RML
Primary TuberculosisPleural Manifestations
Effusion as a manifestation of 1° TBmore common in adults than children
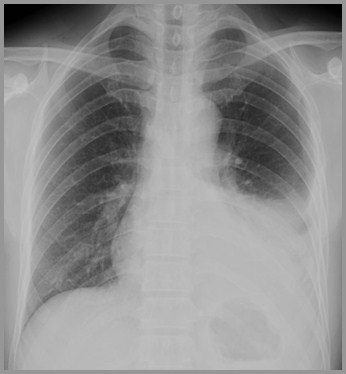
Left Pleural Effusion from Primary TB
Primary TuberculosisGeneral
Calcification in 1° complex is overallrelatively rare
Few patients with 1° TB have clinicalmanifestations
PostprimaryTuberculosisReactivation TB
Reactivation TBGeneral
Most cases in adults occur as reactivation of 1°focus of infection acquired in childhood
Caseous necrosis and tubercle are pathologichallmarks of post 1° TB
Tubercle=accumulations of mononuclearmacrophages, Langhan’s giant cellssurrounded by lymphocytes/fibroblasts
Reactivation TBGeneral
Healing occurs with fibrosis andcontraction
Calcification is rarer than in 1°
Limited mainly to apical and posteriorsegments of upper lobes and superiorsegments of lower lobe
Reactivation TBPatterns
Pneumonia
Cavity formation
Transbronchial spread
Bronchiectasis
Bronchostenosis
Pleural disease
Tuberculoma
Bone involvement
Reactivation TBPatterns
Affects apical or posterior segments ofupper lobes or superior segments of lowerlobes
Bilateral upper lobe disease is verycommon
May present as pneumonia
Cavitation may result
Cavity is usually thin-walled, smooth on innermargin with no air-fluid level

Bilateral Upper Lobe Cavitary Disease withTransbronchial Spread to Lingula
Reactivation TBPatterns
Transbronchial spread may occur—fromone upper lobe to opposite lower
Bronchiectasis—usually asymptomatic
Bronchostenosis due to fibrosis andstricture
Fibrosis may cause distortion of a bronchusand atelectasis many years after initialinfection=“middle lobe syndrome”
Cavitary RUL TB with TransbronchialSpread to LLL
Reactivation TBPatterns
Pleural effusion in postprimary TB
Almost always means direct spread of diseasein to pleural cavity
Should be regarded as an empyema
Carries a graver prognosis than effusion of 1°form
Direct extension into ribs orsternoclavicular joints is uncommon
Solitary pulmonary nodule
Tuberculoma
May occur in either 1° or postprimarydisease
Round or oval lesions with small, discreteshadows in immediate vicinity oflesion=“satellite” lesion
Reactivation TBPatterns
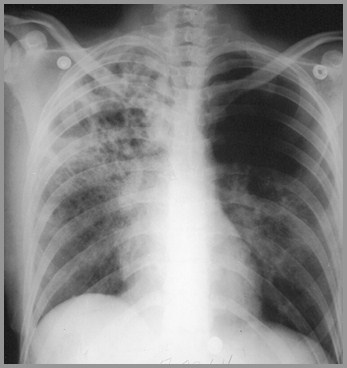
MiliaryTuberculosis
Miliary TuberculosisGeneral
Hematogenous dissemination of bacillicommon in 1° TB but clinically evidentmiliary TB rarely occurs
May not manifest itself for many yearsafter infection
Older men, Blacks and pregnant womensusceptible
Onset is insidious
Fever, chills, night sweats are common
Takes weeks between time ofdissemination and radiographicappearance of disease
Miliary TuberculosisClinical
Miliary TuberculosisNatural History
When first visible, measure about 1 mm insize
Frequently missed on first films
Can grow to 2-3mm if left untreated
When treated, clearing is rapid
Miliary TB does NOT heal with calcification
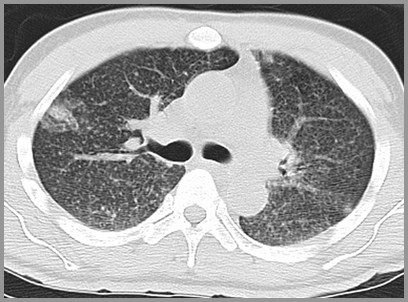
CT of Miliary TB
Calcification in TB3 Funny Names
Ghon lesion=calcified granuloma
Ranke complex=Ghonlesion+calcified lymph node
Simon focus=healed site of 1°infection at lung apex
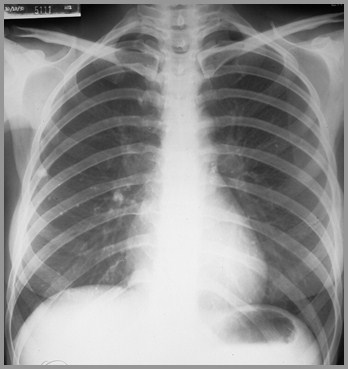
Calcified Hilar Lymph Node and PeripheralGranuloma
TB and Other Diseases
Occurs with a higher incidence in sarcoid-especially if rx with steroids
Associated with silicosis
Associated with HIV infection
No relationship with bronchogenic Ca
TB and AIDS
Mycobacterium avium-intracellulare (MAI)is more common than TB
TB in AIDS looks like 1° form
Hilar and mediastinal adenopathycommon
Cavitation less common
No predilection for apices
TB:The Question of Activity
Only serial images with no change cansuggest lack of activity–2 years
In presence of cavities, activity must bedetermined clinically
TuberculosisAncient Remedies
Rest Theory
“Ping-pong ball” plumbage
Paraffin plumbage
Oleothorax
Pneumothorax andpneumoperitoneum
Thoracoplasty

“Ping-Pong Ball” Plombage in Right UpperLobe

Left-sided Thoracoplasty for TB
The End