
Histiocytosis X
Histiocytosis X
© William Herring, MD, FACR
Histiocytosis XClassification
Letterer-Siwe disease
Hand-Schuller-Christian disease
Eosinophilic Granuloma
Letterer-SiweDisease
Letterer-SiweDisease
Letterer-Siwe DiseaseGeneral
10% of histiocytosis X
Acute disseminated, fulminant form
Age at onset
Several weeks to 2 years
Pathology
May be confused with leukemia
Letterer-Siwe DiseaseClinical
Hemorrhage, purpura
Severe anemia
Fever
Hepatosplenomegaly
Lymphadenopathy
Bone involvement in 50%
Widespread lytic lesions
Letterer-Siwe DiseasePrognosis
70% mortality rate
Hand-Schuller-ChristianDisease
Hand-Schuller-ChristianDisease
Hand-Schuller-ChristianGeneral
15-40% of Histiocytosis X
Age at onset
5-10 years
Pathology
May simulate Ewing'ssarcoma
Hand-Schuller-ChristianClinical
Triad of:
Exopthalmus (33%)
Diabetes insipidus (30-50%)
Lytic skull lesions
Hand-Schuller-ChristianTarget Organs
Bone
Soft tissues
Lung
Hand-Schuller-ChristianBone
Lytic skull lesions with overlying softtissue nodules
Large geographic skull lesions
“Floating teeth” with mandibularinvolvement
Hand-Schuller-ChristianSoft tissue
Hepatosplenomegaly is rare
Common in Letterer-Siwe
Lymphadenopathy may be massive
Hand-Schuller-ChristianLung
Cyst and bleb formation
Spontaneous PTX
EosinophilicGranuloma
EosinophilicGranuloma
Eosinophilic Granuloma
60-80% of Histiocytosis X
Usually confined to bone
Age at onset
5-10 years highestfrequency
Male predominance 3:2
Eosinophilic GranulomaGeneral
Location
Calvarium>mandible>spine>ribs>longbones
Most are monostotic (50-75%)
Eosinophilic GranulomaTarget Organs
Skull50%
Axial skeleton25%
Appendicular skeleton 15%
Lung20%
Eosinophilic GranulomaSkull
Most often diploic space of parietal bone
Round or ovoid punched out lesions withbevelled edge
Bevelled edge=hole-within-a-hole
Sclerotic margin during healing phase
Button sequestrum- bony sequestrumwithin lytic lesion

Beveled Edge Lytic Lesion ofEosinophilic Granuloma
Eosinophilic GranulomaAxial Skeleton
“Vertebra plana”-“coin-on-edge”(Calvedisease)=collapse of vertebral body
Mostly thoracic
Most common cause of vertebra plana inchildren

Vertebra plana in EosinophilicGranuloma
Eosinophilic GranulomaAppendicular Skeleton
Expansile, lytic lesion
Mostly diaphyseal
Soft tissue mass
Laminated periosteal reaction
Eosinophilic GranulomaLung
Age peak between 20-40 years
Multiple small nodules
Predilection for apices
Prototype for honeycomb lung
Recurrent pneumothoraces (25%)
Diffuse Reticular Interstitial Disease inEosinophilic Granuloma

Innumerable thin-walled cysts inEosinophilic Granuloma

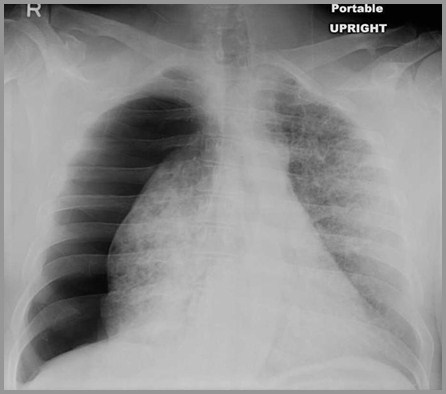
Eosinophilic Granuloma with right-sided tension pneumothorax
Eosinophilic GranulomaNuclear Medicine
Negative bone scans in 35%
Bone lesions usually not Ga-67 avid
Ga-67 may be helpful in detectingnon-osseous lesions
Eosinophilic GranulomaPrognosis
Excellent
The End