
Chest Trauma
Chest Trauma
© William Herring, MD, FACR
What To Look For
Rib fractures
Pulmonary contusions
Pulmonary lacerations
Abnormal collections of air
Abnormal collections of fluid
Rib Fractures
Only important for what they areassociated with or produce
Rib 1 only — facial fractures
Ribs 1, 2 and 3 — Serious Trauma —ruptured bronchus
Ribs 4 – 9 — pneumothorax, contusion
Ribs 10 – 12 — lacerations of liver/spleen
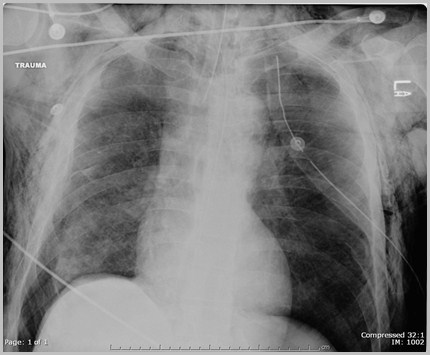
Multiple displaced rib fractures
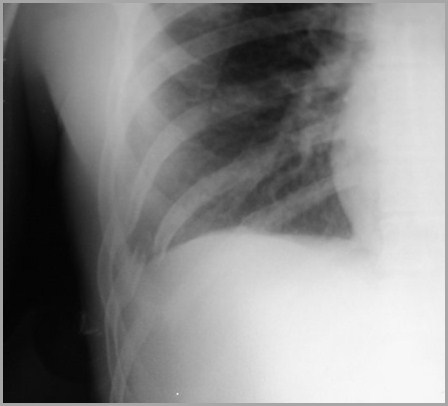
Pulmonary Contusion
Most common finding in blunt chest injury
Hemorrhage into lungs
Appears within 6 hours of injury
Clears in 48 hours
Usually at point of impact
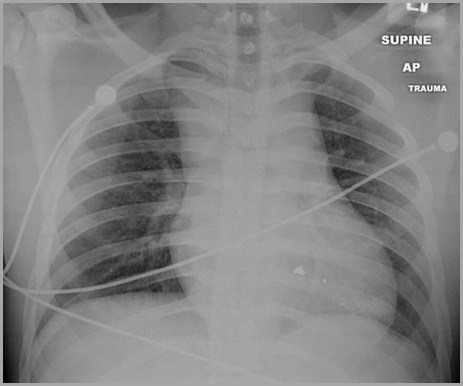
Pulmonary contusion
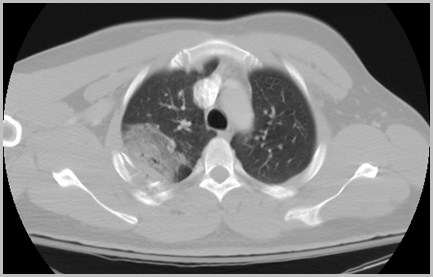
Pulmonary Laceration Traumatic Lung Cyst, Hematoma
Usually not apparent at first because ofsurrounding contusion
Laceration of the lung parenchyma
Usually occurs subpleural under point ofmaximum impact
Half are solid, half are cystic
Takes up to 6 months to clear
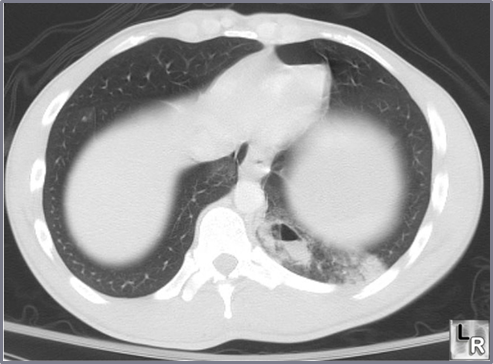
Pulmonary laceration
Abnormal Collections Of Air
Pneumothorax
Pneumomediastinum
Pneumopericardium
Subcutaneous emphysema
Pneumothorax
Must see visceral pleural white line
Absence of lung markings peripheral topleural line
Beware of skin folds
Beware of bullae

Bilateral pneumothoraces
Pneumomediastinum
May develop after blunt trauma due topulmonary interstitial emphysema
Mediastinal pleura is displaced fromheart border
Visualization of central part ofdiaphragm — continuous diaphragmsign
Pneumomediastinum
Pneumopericardium
Requires direct penetration of thepericardium
Air appears around heart but does notextend above great vessels
Very difficult to differentiate frompneumomediastinum

Pneumopericardium
Subcutaneous Emphysema
Streaky air over lateral chest wall orneck
Localized form implies penetratinginjury
Diffuse form associated with pulmonaryinterstitial emphysema
Subcutaneous emphysema
Abnormal Collections of Fluid
Hemothorax
Chylothorax
Hemothorax
Indistinguishable from pleural effusion
Loculation occurs early
Bleeding from parenchyma usually selflimiting
Bleeding from intercostal arteriesproduces enlarging effusions
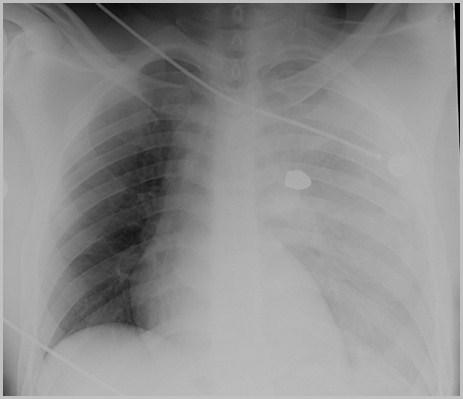
Hemothorax from bullet wound
Chylothorax
Thoracic duct may be torn from blunt orpenetrating injuries
Key is appearance of pleural effusionseveral days after injury
Effusion may occur in either or bothhemithoraces
Pleural tap yields lymph
Signs Of Mediastinal Hemorrhage
Widening of the mediastinum
Subjective, influenced by position
Apical pleural cap on left
Displacement of left paraspinal stripe
Deviation of trachea to right
Deviation of NG tube
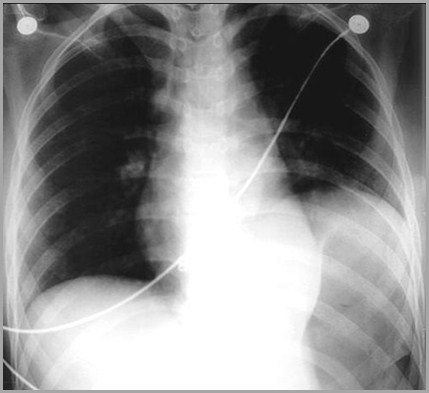
Mediastinal hematoma
Fractures of Trachea and Bronchi
Severe trauma, usually blunt, frequentlyresulting in fxs to ribs 1-3
Mainstem bronchi affected more oftenthan trachea
Fractures of Trachea and Bronchi
Look for large pneumothorax which doesnot respond to suction
Mediastinal or subcutaneous emphysema
Lobar atelectasis, especially developing afew days after trauma
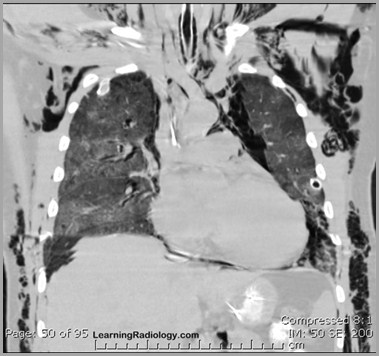
Rupture of the Diaphragm
Left hemidiaphragm affected almostalways
May not occur for weeks after trauma
Hernia may contain omentum, stomach,large and small bowel, spleen, kidney
Rupture of the Diaphragm
X-ray shows bowel, soft tissue at leftlung base
Differentiation from eventration (noconstricted loops) or hernia (nostomach) may be difficult
Ruptured left hemidiaphragm
The End