
Obstructive LesionsTransposition
Obstructive LesionsTransposition
© William Herring, MD, FACR
Transposition ofThe Great Vessels
Transposition ofThe Great Vessels
The Rules
Since anatomic side (i.e. “left” or “right”)in complex lesions is frequently reversedor indeterminate
Naming conventions for
Atria
AV valves
Ventricles
Ventricular outflow tracts
Don’t rely on anatomic side for name
The RulesHow the ventricles are named
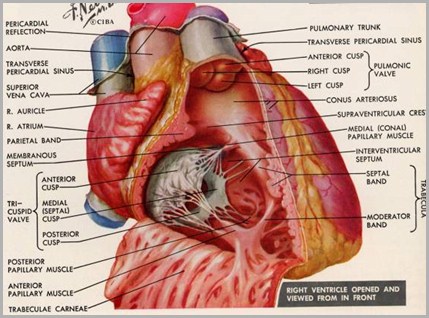
The anatomic right ventricle is thetrabeculated ventricle
The anatomic left ventricle is thesmooth-walled ventricle
The RulesAortic and pulmonic valves
The pulmonic valve is part ofpulmonary artery
Not anatomic right ventricle
The aortic valve is part of aorta
Not anatomic left ventricle
The pulmonic infundibulum is partof anatomic right ventricle
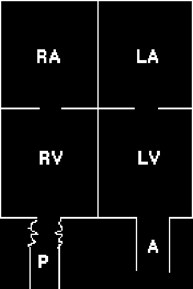
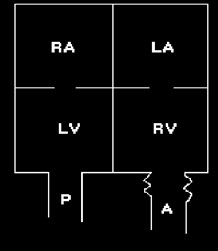
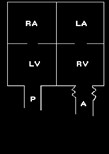
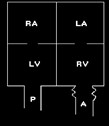
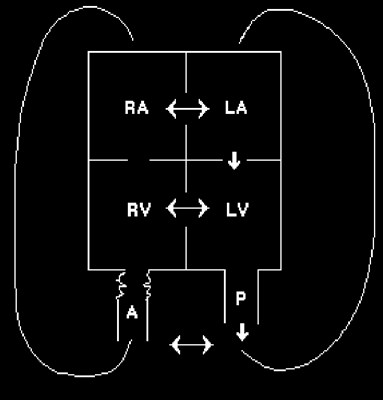
Normal heart
AnatomicRight ventricleis trabeculated
AnatomicLeft ventricle issmooth
Pulmonicinfundibulumalways stays withthe anatomic Rventricle

Ao valvestays withaorta
Pulm valvestays with PA
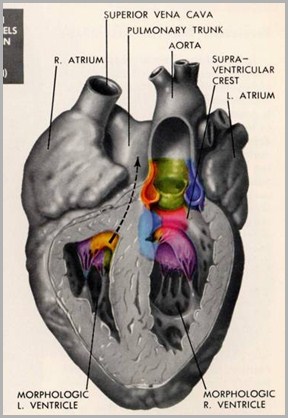
Normal relationship of aortic to pulmonic valves
Pulmonic valve is
Anterior
Lateral
Superior
To the aortic valve
PALS
Normal vs. Transposition
Normal-Pulmonic Valve is
To the Aortic valve
Normal vs. Transposition
Normal-Pulmonic Valve is
Anterior
To the Aortic valve
Normal vs. Transposition
Normal-Pulmonic Valve is
Anterior
Lateral
To the Aortic valve
Normal vs. Transposition
Normal-Pulmonic Valve is
Anterior
Lateral
Superior
To the Aortic valve
Normal vs. Transposition
Normal-Pulmonic Valve is
Transposition-Pulmonic valve is
Anterior
Lateral
Superior
To the Aortic valve
Normal vs. Transposition
Normal-Pulmonic Valve is
Transposition-Pulmonic valve is
Anterior
Posterior
Lateral
Superior
To the Aortic valve
Normal vs. Transposition
Normal-Pulmonic Valve is
Transposition-Pulmonic valve is
Anterior
Posterior
Lateral
Medial
Superior
To the Aortic valve
Normal vs. Transposition
Normal-Pulmonic Valve is
Transposition-Pulmonic valve is
Anterior
Posterior
Lateral
Medial
Superior
Inferior
To the Aortic valve
Corrected Transposition(L-Trans)Inversion of the Ventricles withTransposition of the Great vesselsTwo wrongs do make a right
Corrected Transposition(L-Trans)Inversion of the Ventricles withTransposition of the Great vesselsTwo wrongs do make a right
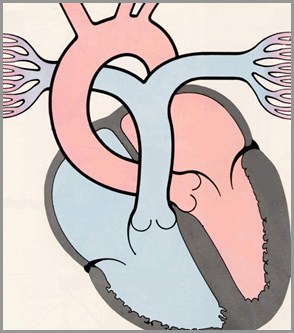
Corrected Transposition (L-Trans)
Inversion of the Ventricles with Transposition of the Great Vessels
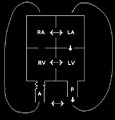
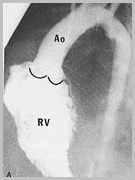
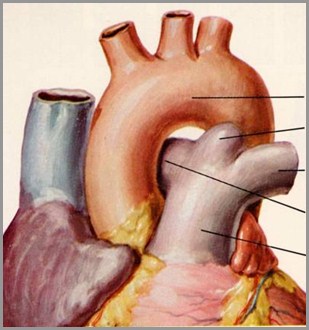
Aorta arisesfrom pulmonicinfundibulum
PA arises fromanatomic leftventricle
Acyanotic
Normalvasculature;or if VSD,then
Ventricles areinverted
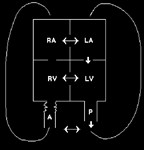
Corrected TranspositionInversion of the Ventricles With TGV (L-Trans)
Physiologically flow is normal
Consistent with normal life, except
Almost always associated with
VSD
Tricuspid valve insufficient (almost 100%)
High incidence of dextrocardia
Complete heart block (conduction systemis inverted)
Corrected TranspositionInversion of the Ventricles With TGV (L-Trans)
Normal to moderately enlarged heart
MPA segment is concave
Waist of the heart is typically narrow
Vasculature is usually of shunt type
Corrected Transposition
Corrected Transposition
R
L
CompleteTransposition of theGreat Vessels(D-Trans)
CompleteTransposition of theGreat Vessels(D-Trans)
Complete TranspositionGeneral
Second most common cardiaccause of cyanosis in infancy
Pulmonary and systemiccirculations form two separatecircuits
There must be mixing between twocircuits for life to continue
Complete TranspositionAssociated abnormalities
About 1/3 have VSD
Larger the shunt, more likely CHF
About ¼ to ½ have patent ductus
Some have ASD
Other major finding is obstruction toblood exiting pulmonary artery
Usually subpulmonic stenosis
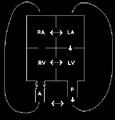
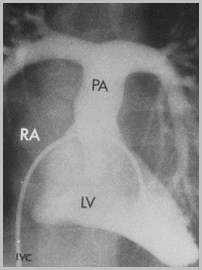
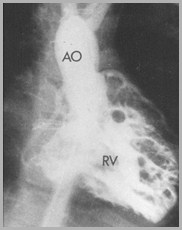
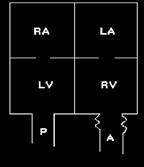
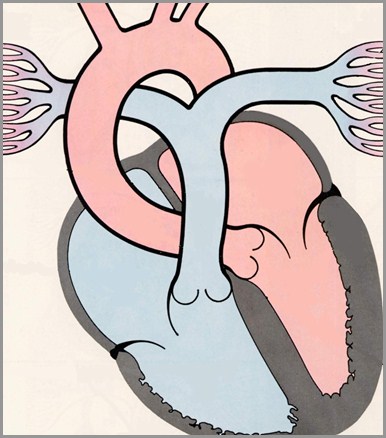
Cyanoticwithincreasedvasculature
Obligatoryshunt sincethere are 2separatecirculations
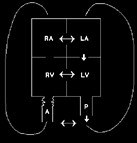
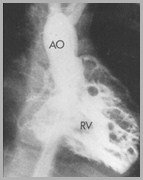
Aorta arisesfrom pulmonicinfundibulum
PA arises fromanatomic leftventricle
ASD
VSD
PDA
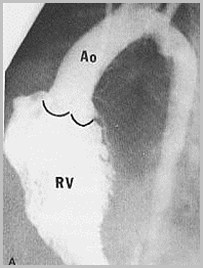
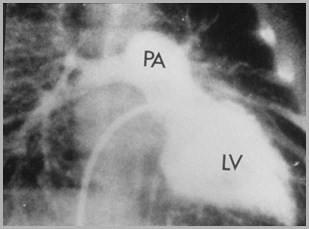
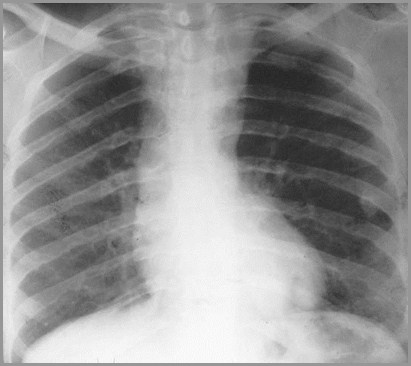
Complete Transposition of the Great Vessels (D-Trans)
Complete TranspositionX-ray findings
Mild cardiomegaly
Concave pulmonary artery segment
Narrow mediastinum (Egg-on-string)
Pulmonary vasculature depends on
Size of shunt and degree of PS
If PS severe & shunt small, vasculature
If PS insignificant & shunt large, vasculature
Why the Mediastinum isNarrow in Transposition
Absence of normal MPA shadow
Aorta frequently ascends straightupward rather than bending to left
Thymus is small or absent from stress
Complete Transposition of the Great Vessels (D-Trans)Cyanotic with Decreased Vasculature
Amersham
Enlargedheart
Narrowwaist
Decreased pulm.vasculature
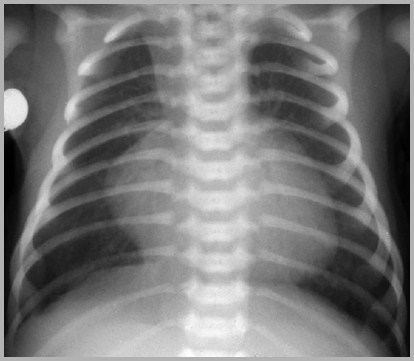
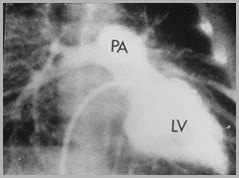
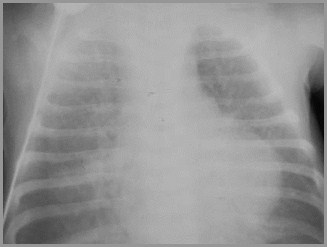
Complete Transposition of the Great Vessels (D-Trans)Cyanotic with Increased Vasculature

Slightly enlargedheart
Increasedvasculature
Increasedvasculature
Concavepulmonary arterysegment
Concavepulmonary arterysegment
Narrowwaist
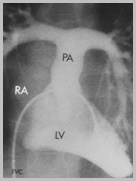
Complete Transposition of the Great Vessels (D-Trans)Cyanotic with Increased Vasculature
Complete Transposition
R
L
Complete Transposition
Corrected Transposition
L
R
R
L

Systemicreturnfrom body
Systemicreturnfrom body
Systemicreturnfrom body
Systemicreturnfrom body
Remembering L from D
Corrected Transposition = normalphysiology = L(iving) Trans
Complete Transposition = abnormalphysiology = D(ead) Trans
ObstructiveLesions
ObstructiveLesions
Lesions ThatCause CHF
Lesions ThatCause CHF
CHF In NewbornImpede Return of Flow to Left Heart
Infantile coarctation
Congenital aortic stenosis
Hypoplastic left heart syndrome
Congenital mitral stenosis
Cor triatriatum
Obstruction to venous return from lungs
TAPVR from below diaphragm
Coarctation of theAorta
Congenital AorticStenosis
Hypoplastic LeftHeart
Congenital MitralStenosis
Cor Triatriatum
Obstruction tovenous return fromlungs
Causes of CHF in the Newborn
Coarctation of theAorta
Congenital AorticStenosis
Hypoplastic LeftHeart
Congenital MitralStenosis
Cor Triatriatum
Obstruction tovenous return fromlungs
Causes of CHF in the Newborn
Diagnosing CHF in a Newborn
Usually have cardiomegaly
Ill-defined bronchovascular bundles
Flattening ofdiaphragm
Air hunger
Rare
Kerley B lines
Pleural effusions
CHF InChronologic Sequence
CHF InChronologic Sequence
Commonest Cause of CHF In Chronologic Sequence
< 24 hrs…………..Intrauterine arrhythmia
First week……….Hypoplastic Left Heart Syndrome
2-6 weeks………..Infantile coarctation
1-4 months………Large L R shunts
VSD, ASD, PDA, AV Canal
CoarctationOf the Aorta
Coarctation of the AortaGeneral
2X more common in males
Common classification
Infantile or preductal form
Adult or juxtaductal form
Adult or juxtaductal (postductal) form ismore common than infantile
Usually localized
Most occur at aortic isthmus
Aortic isthmus = area between LSCA and origin ofductus
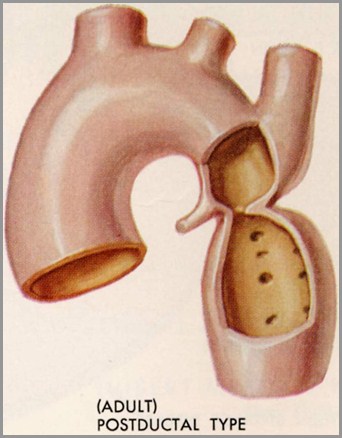
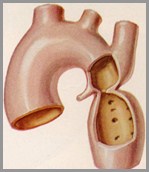
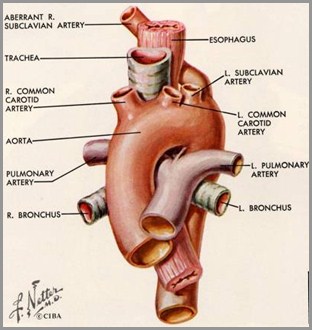
Coarctation of the AortaAdult Form
R Brachiocephalic
L CCA
L SCA
Ductus
“Membrane”arises fromlateralborder ofarch
Coarctation of the Aorta
Heart +/-enlarged
Pre-ductaldilatation
Post-ductaldilatation
Ribnotching
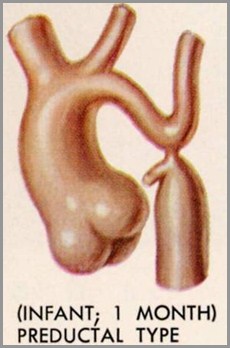
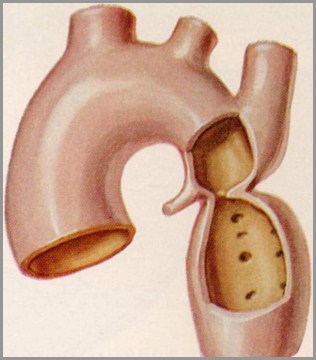
Coarctation of the AortaInfantile Form
Infantile, preductal form = diffuse type
Long, tubular segment of narrowed aorta
From just distal to brachiocephalic artery tolevel of ductus
Intracardiac defects (VSD, ASD, deformedmitral valve) present in 50% of diffuse type
Also patent ductus arteriosis
BCA
LCCA
LSCA
Ductus
Coarctation of the AortaAssociated Defects
Bicuspid aortic valve (most commonassociated defect seen in 50%)
VSD
ASD
Transposition
25% of patients with Turner’s Syndromehave coarctation of aorta
Coarctation of the AortaShone Syndrome
Coarctation of aorta
Aortic stenosis
Parachute mitral valve
Supravalvular mitral ring
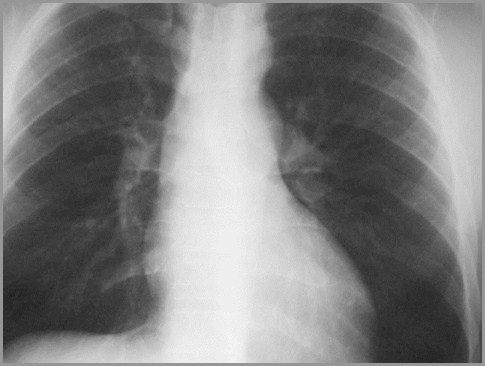
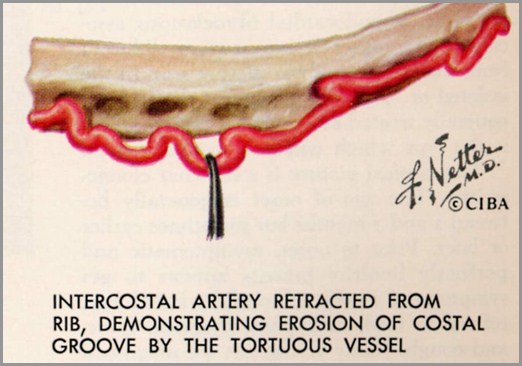
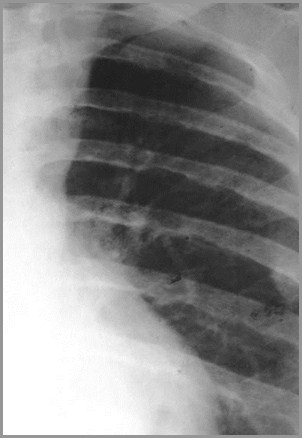
X-Ray FindingsRib Notching
Single best sign
Older the person, more likely to have ribnotching (uncommon <6 yrs)
Majority with coarcts display it >20 yearsof age
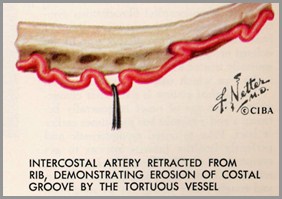
Rib notching occurs in high pressurecircuit
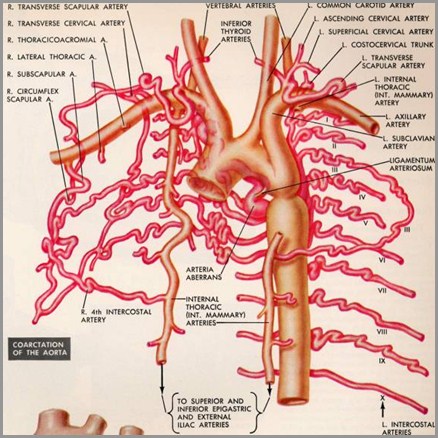
Coarctation of the Aorta
Coarctation of the Aorta
To supply aortadistal to ductus,flow in the 3rd-8thintercostalsreverses
Blood flows fromsubclavian internal mammary intercostals aorta
First twointercostals arisefrom costocervicaltrunk and do notserve aorta
X-Ray FindingsRib Notching
Most often involves 4th-8th rib
Sometimes may involve 3rd and 9th
Does not involve 1st and 2nd ribs
Intercostals come off costocervical trunkand do not supply collateral flow todescending aorta
4th-8th do anastomose with internal mammary toform collaterals for descending aorta
7
Rib Notching inCoarctation
4
5
6
Regresses after coarctis repaired-collateralsdecrease in size on MRI
Costo-vertebraljunction
X-Ray Findings“Figure 3 Sign”
Caused by (in order)
Dilated LSCA or aortic knob
“Tuck” of coarct itself
Poststenotic dilatation
Occurs in 1/3–1/2 of patients with coarct
Not in children
Matched by “reverse 3” or “E” onbarium-filled esophagus

X-Ray FindingsContinued
Convexity of left side of mediastinum justabove aortic knob 2° to
Dilated aorta proximal to coarct, or
Dilated LSCA
May be congenital or may be 2° to pressure
Convexity of ascending aorta in 1/3
May be normal or small in others
Coarctation of the Aorta
Convexityabove aorticknob due todilated LSCAor Aortaproximal tocoarct
AscendingAo may bedilated,normal orsmall
Coarctation of the AortaClinical Findings–Infancy
Severe CHF most common from 2nd to6th week of life
Weak or absent leg pulses
Lower BP in the legs than in the arms
EKG: RV hypertrophy because RVassumes most of the cardiac outputduring fetal life in these patients
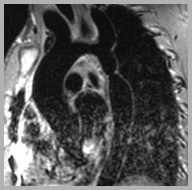
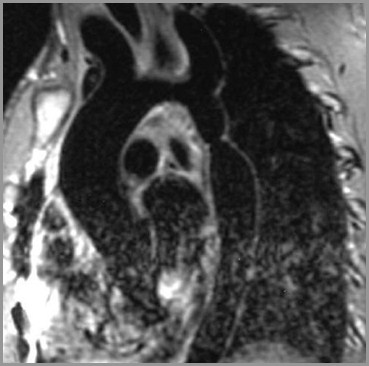
Coarctation of the AortaMRI and Angiography
MRI preferred study in children/adults
Aortography offers greatest resolution


Contrast enhanced MRA shows long segment coarctation of the aorta
Amersham
AO
BCA
Coarct
Oblique sagittal spin-echo-Coarctation of the Aorta
Amersham
Black blood jet from coarctation
University of British Columbia

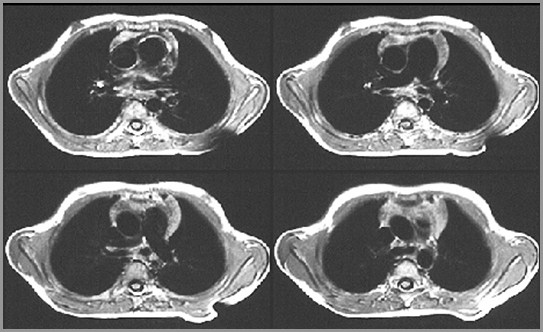
Axial spin-echo MRI-Coarctation of the Aorta
Amersham
Coarctation of the AortaComplications
Heart failure in neonate
Subarachnoid bleeds 2° ruptured Berryaneurysms
Dissection of aorta
Bacterial endocarditis
Mycotic aneurysm
X-Ray FindingsRib Notching–Unilateral
Rib notching occurs in the highpressure circuitProximal to coarctation
Unilateral Rib NotchingRight
HighPressureCircuit
BCA
LCA
LSCA
Ductus
Notching occurs in thehigh pressure circuit
Isolated right-sidedrib notching
Coarct originatesbetween the LCCAand the LSCA
Unilateral Rib NotchingLeft
HighPressureCircuitHighPressureCircuit
Notching occurs in thehigh pressure circuit
Isolated left-sidedrib notching
Anomalous RSCAoriginates distalto site of coarct
Pseudocoarctation
Buckling of aorta resembles truecoarctation
No pressure gradient (<30mmHg)
Figure 3 sign present
No rib notching

Pseudocoarctation
Coarctation of theAorta
Congenital AorticStenosis
Hypoplastic LeftHeart
Congenital MitralStenosis
Cor Triatriatum
Obstruction tovenous return fromlungs
Causes of CHF in the Newborn
9
2
The End