
The Heart:Inside Out
© William Herring, MD, FACR
Intraluminal Lesions
Tumors andThrombi
Cardiac Tumors
Rare
Metastatic tumors are 20x morecommon than primary tumors
Melanoma, lymphoma, lung and breastmost frequent
Most mets involve the pericardium
Cardiac Tumors
In children, most common tumor isrhabdomyoma
In adults, most common benign tumoris myxoma
Angiosarcoma most common 1° malignant
Usually right-sided
Myxomas
Most common 1° benign cardiac tumor
Usually found in left atrium
Arise from inter-atrial septum
About 10% calcify
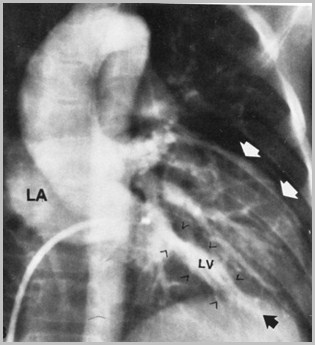
Myxoma in Left Atrium

©Miller-Requisites
©Miller-Requisites
Thrombi ─ Ventricular
In left ventricle
After MI
In a ventricular aneurysm
Filling defects in opacified cardiacchamber
May calcify
Thrombi ─ Ventricular
Occur on cardiac walls that are akinetic
Usually at cardiac apex or along IV septum
Biggest pitfall
May be confused with posterior papillarymuscles
Look for thickened chordae

Thrombus in Right Ventricle
Thrombi ─ Atrial
Commonly associated with LAenlargement
Most frequent in mitral stenosis withatrial fibrillation
Left atrial appendage a frequent site
Thrombus in left atrial appendage
Myocardium
Cardiomyopathy
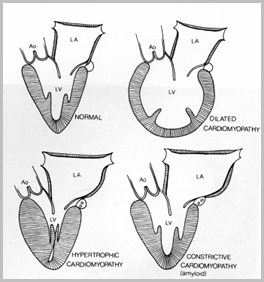
Classification
Dilated cardiomyopathy
Restrictivecardiomyopathy
Hypertrophiccardiomyopathy
Arrhythmogenic rightventricular dysplasia
©Elliot-CardiacImaging
©Elliot-CardiacImaging
DilatedCardiomyopathy
DilatedCardiomyopathy
Dilated Cardiomyopathy
More than 1/2 of patients are alcoholics
Dilatation of both ventricular cavities
Over 75% have mural thrombi
Most often LV > RV > RA > LA

Dilated CardiomyopathyOther Causes
Idiopathic
Coronary artery disease
Myocarditis
Lupus
Viral infection
Dilated CardiomyopathyClinical
Severe, intractable CHF is dominantsymptom
Usual cause of death
Poor systolic ventricular function
Leads to thrombogenesis
Cardiomegaly
Usually involves left ventricle
CHF is very common
Echo: poor global wall motion
Wall thickness usually thin
Dilated CardiomyopathyImaging Findings
Dilated Cardiomyopathy
Classification
Dilated cardiomyopathy
Restrictivecardiomyopathy
Hypertrophiccardiomyopathy
Arrhythmogenic rightventricular dysplasia
©Elliot-Cardiac Imaging
©Elliot-Cardiac Imaging
RestrictiveCardiomyopathy
RestrictiveCardiomyopathy
Restrictive CardiomyopathyGeneral
Least common cardiomyopathy
Normal ventricular size
Problem is inability of ventricles to fillproperly
Thick LV wall and dilated LA

Mural thrombi ─ occasionally
Resembles constrictive pericarditis
Biopsy may be needed
Restrictive CardiomyopathyGeneral
Restrictive CardiomyopathyCauses
Associated with extracellular infiltration
Amyloid
Sarcoid
Glycogen storage diseases
Mets
Radiation
Restrictive CardiomyopathyImaging Findings
Mild cardiomegaly
Walls are stiffened
CHF is common
Echo: Normal-sized LV cavity
Dilated left atrium
Pericardium not thickened vs.constrictive pericarditis

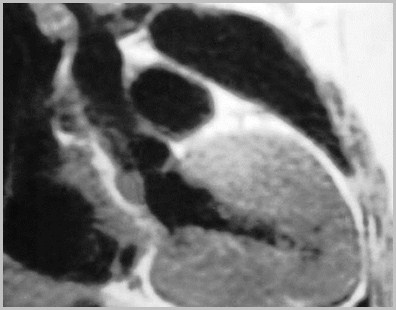
ECG-gated spin-echo image - enlargementof both atria and normal size ofventricles with thickened walls
Amersham
Restrictive cardiomyopathy
Classification
Dilated cardiomyopathy
Restrictivecardiomyopathy
Hypertrophiccardiomyopathy
Arrhythmogenic rightventricular dysplasia
©Elliot-Cardiac Imaging
©Elliot-Cardiac Imaging
HypertrophicCardiomyopathy(HCM)
HypertrophicCardiomyopathy(HCM)
Severe LV, and sometimes RV,hypertrophy
Thickened IV septum
No ventricular enlargement at first
Divided into primary and secondary
Further divided into those with andwithout LVOT obstruction

Hypertrophic CardiomyopathyIdiopathic Hypertrophic Subaortic Stenosis
Genetic
Autosomal dominant with variable penetrance
Hypertrophy may be concentric orlocalized
Asymmetric septal hypertrophy (ASH)
IV septum is 1.5x thicker than posterior LV wall
Disproportionate upper septalthickening (DUST)
Hypertrophic CardiomyopathyPrimary
Hypertrophic CardiomyopathyPrimary
May present from birth to old age
Common cause of sudden cardiacdeath in patients < 40 yrs old
Most common cause of death amongstcompetitive athletes
About 2/3 do not have LVOTobstruction
Unlike Dilated Cardiomyopathy which ishypokinetic, HCM is hyperkinetic
LV empties too completely
Atria attempt to compensate and enlarge
Much larger atria than in DilatedCardiomyopathy
Hypertrophic CardiomyopathyPrimary
Hypertrophic CardiomyopathySecondary, Non-obstructive
Non-obstructive hypertrophiccardiomyopathy (HCM) is common
Seen with high blood pressure
Concentric and uniform thickening of LVwall
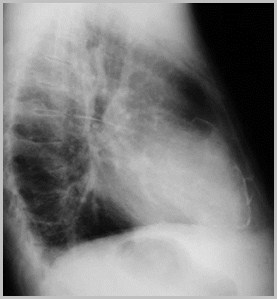
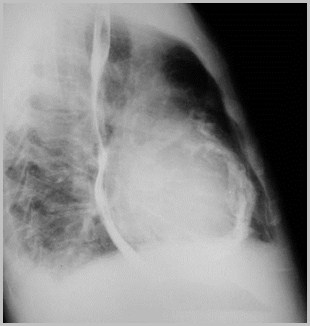
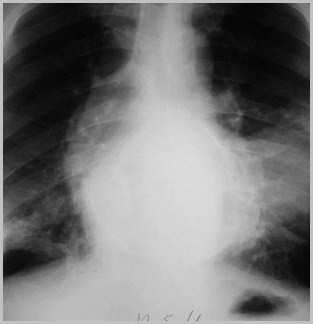
Hypertensive cardiovascular disease
Uncoiledaorta
Uncoiledaorta
ProminentLV
ProminentLV
Hypertrophic CardiomyopathyObstructive (HOCM)
Hallmark of HOCM: dynamic subvalvularaortic stenosis
Anterior leaflet of mitral valve moves intoLVOT on systole and obstructs it
Systolic Anterior Motion (SAM) of mitral valve
Hypertrophic CardiomyopathyObstructive (HOCM)
Neither ASH nor SAM is specific for HOCM
E.g. ASH also seen in Pulmonic Stenosis
SAM also seen in Transposition of Great Vessels
Hypertrophic CardiomyopathyImaging Findings
Usually normal-sized heart
Left atrium may be enlarged 2° MR
CHF is not common
Echo: LV hypertrophy
ASH
Dynamic LVOT obstruction
SAM
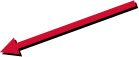
ECG-gated spin-echo image incoronal plane - severe symmetrical hypertrophy of LV
Hypertrophic Cardiomyopathy
Amersham
Hypertrophic Cardiomyopathy
Amersham
©Miller-Requisites
©Miller-Requisites
Thickenedapex
Thickenedapex
Asymmetric septal hypertrophy
Asymmetric septal hypertrophy
Hypertrophic Cardiomyopathy
Markedwallthickening
Markedwallthickening
MitralRegurgitation
From SAM
MitralRegurgitation
From SAM
©Elliot-Cardiac Imaging
©Elliot-Cardiac Imaging
Almostcompleteemptying ofLV
Almostcompleteemptying ofLV
Dilated
Restrictive
Hypertrophic
LV Cavity Size
Increased
Normal
Normal
MitralRegurgitation
Mild
Variable
HOCM: mild tosevere
Wall motion
Global hypokinesis
Normal
Hyperkinetic
Mural thrombi
Frequent
Occasional
None
Systolic Function
Decreased
Normal
Increased
Diastolic Function
Normal
Decreased
Normal
Ejection Fraction
Decreased
Normal
Normal
Classification
Dilated cardiomyopathy
Restrictivecardiomyopathy
Hypertrophiccardiomyopathy
Arrhythmogenic rightventricular dysplasia
©Elliot-Cardiac Imaging
©Elliot-Cardiac Imaging
Arrhythmogenic RightVentricular Dysplasia
Rare cardiomyopathy
Arrythmias and sudden death
Younger age group
RV anterior free wall replaced by fat andfibrous tissue
Thinning of ant wall; more fat than normal
Dilated RV, aneurysms and tricuspidregurgitation
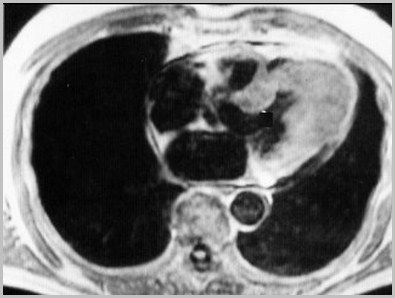
Arrhythmogenic RightVentricular Dysplasia
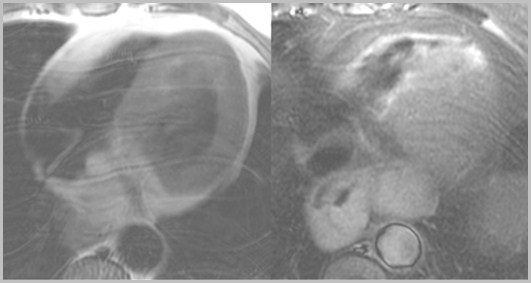
Left-thickening and replacement of RV anterior wall by fatty tissue.Fat suppression (right) - loss of signal in RV anterior wall, confirmingfatty nature of these changes
Left-thickening and replacement of RV anterior wall by fatty tissue.Fat suppression (right) - loss of signal in RV anterior wall, confirmingfatty nature of these changes

Endocarditis
EndocarditisGeneral
Triad: fever, murmur, septicemia
Causes
Rheumatic fever
Infection
Non-bacterial thrombotic endocarditis
Libman-Sacks Endocarditis
Smaller vegetations than bacterial
EndocarditisGeneral
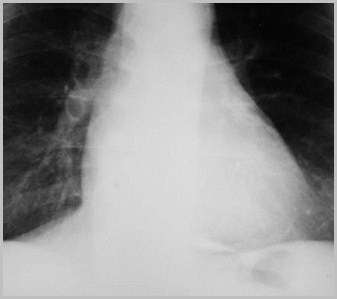
Vegetations frequently produceregurgitation of affected valve
Can embolize to lungs or aorta
Septic emboli in lungs
May produce mycotic aneurysm of aorta
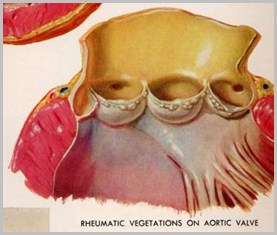
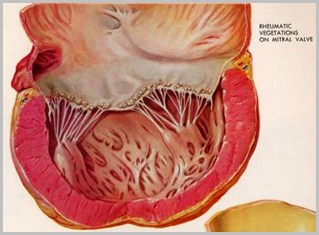
Rheumatic Vegetations
Rheumatic Vegetations
© Frank Netter, MD Novartis®
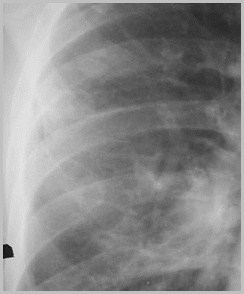

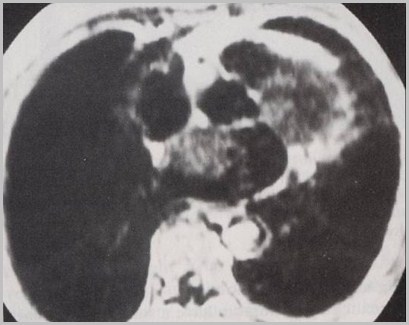
Septic Emboli to Lungs
Septic Emboli to Lungs
Septic Emboli to Lungs
Septic Emboli to Lungs

Pericardium
Pericardium
Pericarditis
Pericarditis
Constrictive Pericarditis
Thickening of pericardium impedingdiastolic filling
Thickened pericardium may calcify
Right-sided failure due to impeded RVfilling
Constrictive PericarditisCauses
Viral pericarditis (most common)
Tuberculous pericarditis
Uremic pericarditis
Post-cardiac surgery
Constrictive PericarditisCalcification
Calcified pericardium doesn’t implyconstriction
About 50% with constrictive pericarditiscalcify
About 50% of calcified pericardiums arevisible on CXR
Constrictive PericarditisCalcification
Types of calcification
Eggshell – viral and uremic
Shaggy, amorphous in AV grooves – TB
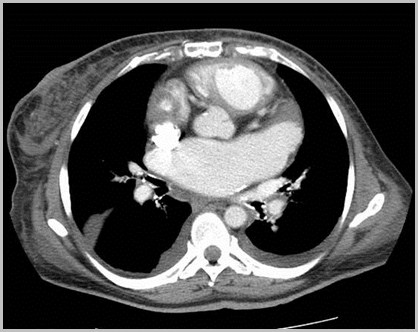
Constrictive PericarditisEggshell calcification as seen in viral or uremic pericarditis
Constrictive PericarditisThick calcification as seen in Tuberculous pericarditis
Constrictive Pericarditis vs.Restrictive Cardiomyopathy
Both have abnormal filling of the heart
May be impossible to distinguish two
CT best for calcified pericardium
If calcified, not restrictive cardiomyopathy
Normal pericardium on both CT and MRI
Excludes constrictive pericarditis
Constrictive Pericarditis
Restrictive Cardiomyopathy
Heart size
Normal
Normal
Pericardial Calcification
Present
Absent
Constrictive Pericarditis vs.Restrictive Cardiomyopathy
Congenital Defect inthe Pericardium
Congenital Defect inthe Pericardium
Premature atrophy of left duct of Cuvier(cardinal vein)
Failure of nourishment of left pleuro-pericardial membrane failure ofpericardium to develop
Congenital Pericardial DefectEmbryogenesis
Congenital Pericardial DefectGeneral
Male:female ratio of 3:1
May be detected at any age
Most common in low 20’s
Congenital Pericardial DefectLocation
Foraminal defect on left side 35%
Complete absence of left side35%gives levoposition of heart
Diaphragmatic surface 17%
Total bilateral absence9%
Right sided4%
Congenital Pericardial DefectAssociations
Bronchogenic cysts
VSD, PDA, mitral stenosis
Diaphragmatic hernia
Sequestration
Congenital Pericardial DefectClinical
Mostly asymptomatic
May have:
Tachycardia
Palpitations
Right bundle block
Positional discomfort lying on left side
Chest pain
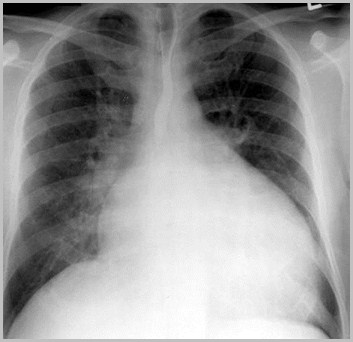
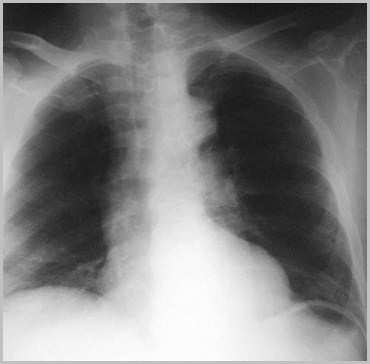
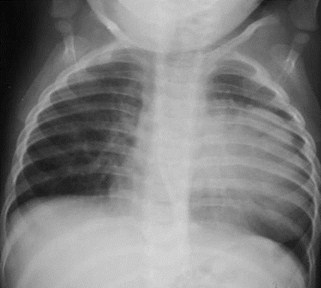
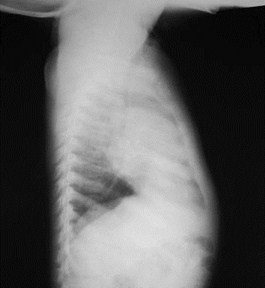
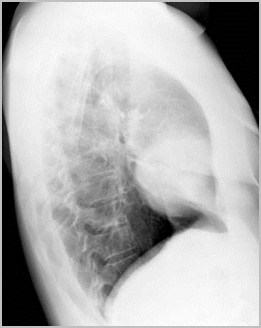
Congenital Pericardial DefectX-ray Findings
Focal bulge in area of main pulmonaryartery
Sharply marginated
Lung may interpose between heart-lefthemidiaphragm
Increased distance between sternum andheart 2° absence of sternopericardialligament
Levoposition of heart
Pneumopericardium followingpneumothorax
Congenital Pericardial DefectX-ray Findings-Continued
Congenital Defect in the Pericardium
Congenital Defect in the Pericardium

Congenital Pericardial DefectTreatment
Since herniation and strangulation ofleft atrial appendage or herniation ofLA/LV may occur
Foraminal defect requires surgery
The End
The End