|
|
Inflammatory Polyps of the Esophagus
General Considerations
- Uncommon polypoid lesions of the esophagus
- Most common mucosal lesion: squamous papilloma
- Most common submucosal lesion: leiomyoma
- Nearly all occur in the distal esophagus or esophagogastric junction
- Frequently associated with erosive esophagitis or ulcer
- No malignant potential reported
- These have also been called “sentinel fold” or inflammatory pseudopolyps, but terminology is confusing (see box below)
Clinical Findings
- Associated with gastroesophageal reflux and reflux esophagitis
- Usually found incidentally, though, unless they are large when they can cause dysphagia or bleed
Imaging Findings
- Seen on barium swallows as either radiolucent filling defects in the barium pool or as barium-etched lines within the esophageal lumen.
- Smooth-surfaced enlargements atop a thickened rugal fold at the gastric cardia
- Frequently seen when the esophagus is collapsed
Differential Diagnosis
Differential Diagnosis of Polypoid Esophageal Lesions |
Lesion |
Remarks |
Fibrovascular polyps |
Referred to as fibromas, fibrolipomas, myomas, and lipomas; they are differentiated by their mixture of fibrous, vascular, and adipose tissue covered by squamous epithelium. They are quite rare and are most commonly encountered in the upper third of the esophagus and typically attach directly to the inferior aspect of the cricopharyngeus. About 75 percent of cases have been reported in men in their fifties or sixties.
Fibrovascular polyps do not generally cause symptoms. However, case reports have described prolapse of large lesions into the larynx causing asphyxiation; lesions as large as 20 cm have been reported. Other symptoms associated with large lesions include dysphagia, chronic cough, nausea, and vomiting. Polyps that extend into the proximal stomach are exposed to an acidic environment, which can lead to ulceration and bleeding.
Symptomatic polyps often have a stalk, allowing them to be removed endoscopically using a snare. |
Adenomas |
Esophageal adenomas arise almost exclusively in segments of Barrett's esophagus and likely represent a polypoid or nodular form of dysplasia rather than an isolated polypoid adenoma. The association with Barrett's esophagus is further supported by the concomitant finding of esophageal adenocarcinoma in many patients.
Isolated lesions without associated Barrett's smaller than 1 cm may be resected endoscopically using a biopsy forceps or snare. Lesions larger than 1 cm and those containing high-grade dysplasia can be removed using endoscopic mucosal resection, whereas more advanced lesions may require surgery.
|
Inflammatory fibroid polyps |
Inflammatory fibroid polyps describe a variety of lesions that are composed of reparative tissue with reactive blood vessels, fibroblasts, and inflammatory cells including hamartomas, inflammatory pseudopolyps, and eosinophilic granulomas.
They are rare, with only one case found in 330,000 surgical specimens submitted in one hospital over 60 years. They are more commonly found in the stomach, small bowel, and colon than the esophagus.
They are thought to occur primarily from acid reflux-induced inflammation, a theory supported by their occurrence mainly in the distal esophagus, including the gastroesophageal junction.
Inflammatory fibroid polyps are considered to be benign, reactive inflammatory lesions whose defining histologic features include a connective tissue stroma and a diffuse eosinophilic infiltrate. They generally are an incidental finding but can occasionally cause hemorrhage or dysphagia. |
Papillomas |
Papillomas are benign epithelial lesions characterized histologically by fingerlike projections of tissue lined by an increased number of squamous cells and a core of connective tissue that contains small blood vessels.
They are rare; their incidence in patients undergoing upper endoscopy has ranged from 0.01 to 0.45 percent, while their prevalence in the general population based on autopsy series ranged from 0.006 to 0.04 percent.
The pathogenesis of esophageal papillomas is uncertain but several lines of evidence support an underlying inflammatory condition. Approximately 70 percent of papillomas occur in the distal one-third of the esophagus, and have been associated with documented reflux, esophagitis, or mucosal irritants such as nasogastric tubes. There is also evidence to support a role of human papilloma virus (HPV) in the formation of esophageal papillomas.
Esophageal papillomas have been most commonly diagnosed in patients who are in their 50s. Some studies suggest they are more common in men (male to female ratio of 1.8-3.4 in various reports), while others have reported an equal sex distribution.
The majority of papillomas are solitary. They can be seen more frequently in patients with tylosis and acanthosis nigricans and there is an association with Goltz syndrome, a congenital disorder of focal dermal hypoplasia that features hyperpigmentation, sclerodactyly, dysplastic changes of the teeth and bones, and perianal, oroesophageal, and genital papillomas.
Most lesions do not cause symptoms, but large lesions can cause dysphagia. Papillomas can generally be resected endoscopically. Lesions smaller than 1 cm can usually be removed with a cold-forceps biopsy, but larger lesions require endoscopic mucosal resection. |
From Benign Lesions of the Esophagus. D Wild and M Guelrud. Up to Date. |
Treatment
- A standard biopsy generally provides enough tissue to make a diagnosis.
- Resection is not necessary except for lesions that cause symptoms, which may warrant snare polypectomy or surgical resection.

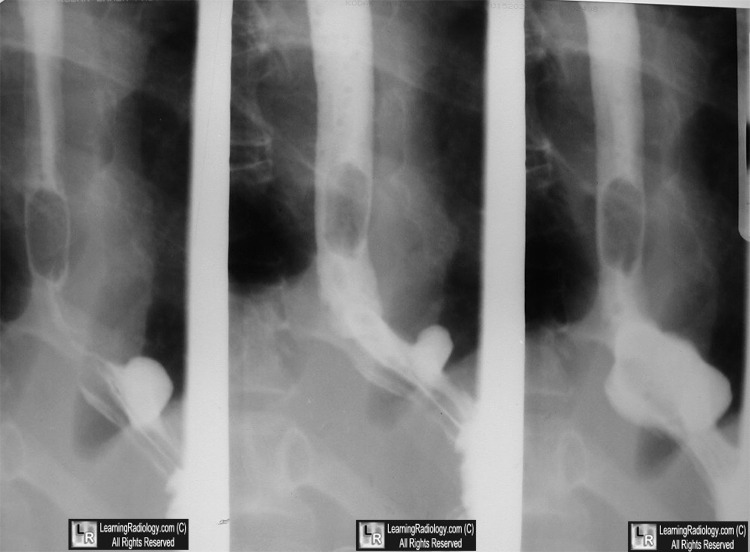
Inflammatory Polyp of the Esophagus. Three images from a barium esophagram show a smoothly-marginated, well-circumscribed, persistent filling defect in the lower esophagus (white arrows) near the esophagogastric junction with the suggestion of a rugal fold emanating from the stomach ending in the polyp.
For this same photo without the arrows, click here
For more information, click on the link if you see this icon 
Differential diagnosis of esophageal disease on esophagography. SE Rubesin and MS Levine. Applied Radiology. Vol. 30,
Number 10, October 2001
Benign Lesions of the Esophagus. D Wild and M Guelrud. Up to Date.
|
|
|

{kind=link}