|
|
Interruption of the Inferior Vena Cava
With Azygos Continuation
General Considerations
- Rare
- Frequently associated with other congenital anomalies
- Occurs in 0.6% of patients with congenital heart defects
- In usual form, the IVC is interrupted above level of renal veins
- There is absence of the hepatic segment of the IVC and the post-renal IVC continues as azygos and hemiazygos veins
- Embryologically, there is a failure to form right subcardinal–hepatic anastomosis resulting in atrophy of right subcardinal vein
Clinical Findings
- Usually asymptomatic from vascular anomaly itself
- May have venous insufficiency of lower extremities
- Other symptoms related to associated congenital abnormalities (congenital heart disease)
Imaging Findings
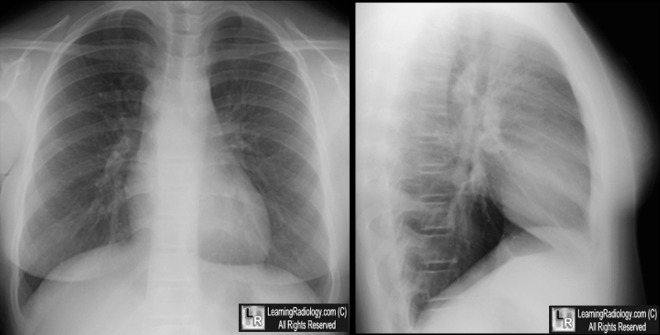
- Conventional Radiographs
- Soft tissue density with smooth, well marginated outer border at junction of the trachea and right main bronchus
- Normal azygos vein is about 1.0 cm in size in upright position and 1.5 cm in supine position
- Size of azygos vein will increase in supine position and decrease in upright position or during Valsalva maneuver
- Absence of the normal triangular shadow of the IVC posteriorly at the base of the heart on the lateral view (at times)
- Prominence of aortic nipple
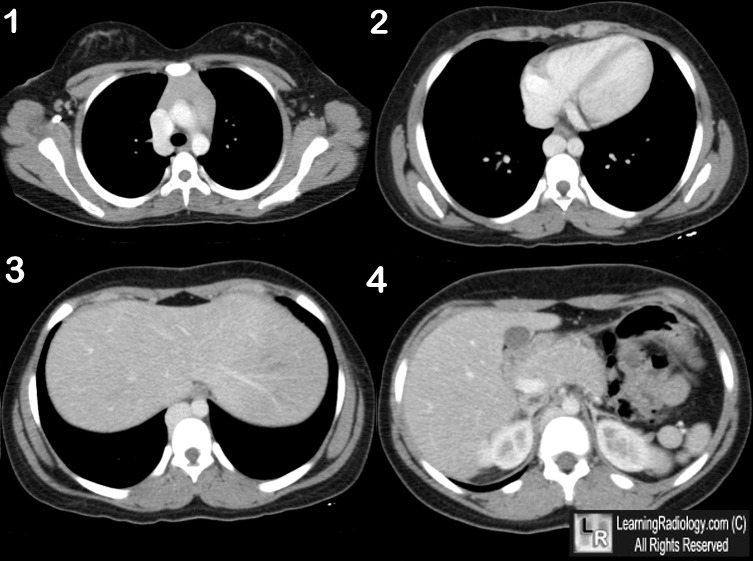
- CT
- Large, tubular posterior structure either dilated azygos (on right) or hemiazygos (on left)
- IVC passes posterior to diaphragmatic crus to enter thorax as azygos vein
- Azygos vein joins superior vena cava at normal location in right peribronchial location
- Enlarged azygos vein is similar in attenuation to superior vena cava
- Gonadal veins drain to ipsilateral renal veins
Differential Diagnosis
- Mediastinal mass (e.g., lymphadenopathy)
- Right-sided aortic arch
- Acquired obstruction of the IVC or SVC
Treatment
- None usually required except as related to associated congenital abnormalities
Complications
- May affect interventional procedures (IVC filter placement)
- May affect surgical procedures (esophagectomy, liver transplants)
- Congenital heart defects
- Most often AV canal, PAPVR, ASD, VSD, double outlet right ventricle
- Polysplenia and situs abnormalities
- Truncated pancreas
- Intestinal malrotation


Interruption of Inferior Vena Cava (IVC)
with Azygos Continuation. Upper: Frontal chest radiograph shows a soft tissue mass at the tracheobronchial angle with a smooth margin (white arrow). A tubular structure descends to the right of the spine (yellow arrows). The aorta is on the left. The lateral view does show a retrocardiac triangular density consistent with an IVC. Lower: Serial, contrast-enhanced CT scans of the chest and upper abdomen show an enlarged azygos vein (yellow arrow) that descends to the right of the aorta. There is no intrahepatic IVC. The liver is midline (black arrow). There are multiple spleens present (polysplenia) (yellow circle).
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
Congenital Interruption of the inferior vena cava. RL van der Horst and AR Hastreiter. Chest 1981;80;638-64
|
|
|

{kind=link}
{kind=link}