|
|
Hydatidiform Mole
Submitted by Peachy Mae Piana, MSIV
General Considerations
- Hydatidiform mole is the most common form of gestational trophoblastic disease
- Two types of moles
- Complete mole
- Occurs when an empty ovum is fertilized with a sperm
- Diploid (paternal DNA only)
- No coexistent fetus
- 15% risk of progressing to persistent gestational trophoblastic neoplasia
- Partial mole
- Occurs after two sperm fertilize a normal ovum
- Triploid (maternal and paternal DNA)
- Nearly always with a coexistent fetus
- 3% risk of progressing to persistent gestational trophoblastic neoplasia
- Risk factors
- Asian and Native American women
- Mothers under age 20 years and mothers over age 35
- Previous molar gestation and spontaneous abortions
Clinical Findings
- Classic clinical triad
- Uterine enlargement inconsistent with dates
- Hyperemesis gravidarum
- Markedly elevated serum hCG level
- Other clinical manifestations include vaginal bleeding, pelvic pain, hyperthyroidism, preeclampsia, and respiratory distress syndrome
Imaging Findings
- Ultrasound is primarily used to rule out an intrauterine pregnancy
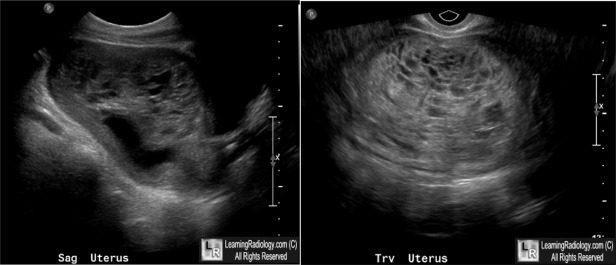
- Classic sonographic appearance of a complete mole
- “Snowstorm” or “granular” appearance
- Central heterogeneous mass with numerous anechoic (cystic) spaces
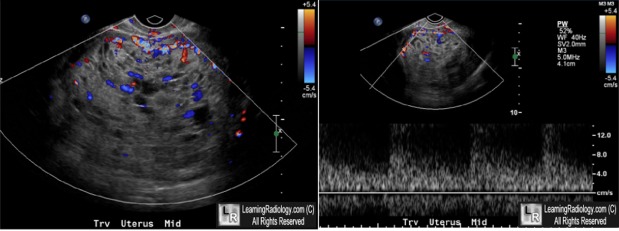
- Low resistance arterial and venous flow
- Absence of embryo or fetus
- When sonographic appearance and hCG levels are suspicious for hydatidiform mole, the diagnosis should be confirmed by histology
Differential Diagnosis
- Partial Mole
- Missed abortion
- Choriocarcinoma
Treatment
- Treatment involves evacuation of uterine contents by dilation and curettage
- Alternatively, patients who do not desire further fertility may opt for a hysterectomy to prevent local invasion.
Complications
- Choriocarcinoma
- Invasive Mole

Complete Mole. Transabdominal and transvaginal sonographs show an enlarged uterus
containing a large echogenic mass (yellow dotted line) with innumerable anechoic (cystic) spaces (green arrows).
Vascular flow is seen during systole (open red arrow) and diastole (closed red arrow),
representing low resistance flow within this mass. No intrauterine gestation is seen.
In combination with an extremely elevated beta-hCG, these findings are concerning for a complete molar pregnancy.
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
Soper, J. Surgical therapy for gestational trophoblastic disease. J Reprod Med 1994; 39: 168.
Michael Novick, Evan H. Dilon, Neal Epstein. AJR Teaching File: Pregnant Woman With Vaginal Spotting, Nausea, and Vomiting. AJR:194, June 2010.
Brent Wagner, Maj USAF, MC, Paula Woodland, MD, Glenn Dickey, Lt. Col, USAF, MC. Gestational Trophoblastic Disease: Radiologic-Pathologic Correlation. Radiographics. Vol 16. Number 1. January 1996
|
|
|

{kind=link}
{kind=link}