|
|
Osler-Weber-Rendu Disease
Hereditary Hemorrhagic Telangiectasia
- General considerations
- Also known as hereditary hemorrhagic telangiectasia (HHT) and Rendu-Osler-Weber syndrome
- It is a disease characterized by mucosal and cutaneous telangiectasias and arteriovenous malformations (AVMs)
- Oddly enough, Osler-Weber-Rendu Disease (OWRD) was first described by Sutton in 1864 but, alas, Sutton’s name is not on the disease
- The disease is named after Henri Rendu (1896), Sir William Osler (1901) and Frederick Parks Weber (1907) who described various aspects of the syndrome in the years cited
- Pronounced OHz-ler, ren-DYU, and VAY-ber (Germanic pronunciation of his name)
- It is autosomal dominant with variable penetrance
- Most frequent cause maps to the long arm of chromosome 9
- Affects both sexes evenly
- May present at any age but most commonly in third decade
- Pulmonary AVMs can bleed in early childhood
- GI bleeds typically occur later, in 4th-5th decades
- Classical triad
- Telangiectasia
- Typically smaller than 5 mm
- Recurrent epistaxis (most common presentation)
- Positive family history
- First-degree relative with the disease
- Also, multi-organ arteriovenous malformations (AVMs) and aneurysms
- Manifestations of disease are secondary to bleeding from these AVMs
- By the numbers
- Overall, 60% of patients with pulmonary AVMs have OWRD
- 20% of patients with OWRD have a pulmonary AVM
- Imaging findings
- Pulmonary AVMs may appear as a solitary or multiple masses with thick, rope-like densities (vessels) leading back to the hilum
- CT is best as demonstrating these lesions
- Hepatic AVMs appear as large pools of contrast with intervening enlarged hepatic vessels
- CNS AVMs may be shown better on MRI
- Clinical findings
- Epistaxis
- Fatigue
- Dyspnea on exertion
- Cyanosis
- Clubbing
- Polycythemia
- Neurologic signs and symptoms from stroke, brain abscess or TIA
- Complications
- Risk of hemorrhage from nasal mucosa
- Pulmonary hemorrhage
- High output cardiac failure
- Uncommon, from large left-right shunt
- Stroke
- Hemorrhagic strokes are secondary to cerebral AVMs
- Ischemic strokes are secondary to pulmonary AVMs
- Migraines
- Mechanism is unknown but they are frequently associated with pulmonary AVMs
- Paradoxical emboli
- Emboli arising from right side of body pass unfettered through the lung AVM to the left-sided circulation
- Brain abscesses
- Normal pulmonary capillary filtering mechanism is not present in those with pulmonary AVMs
- Pulmonary involvement
- Probably the most significant in terms of its consequences
- Pulmonary AVMs produce right-to-left shunts which allow for emboli originating from the venous system to reach systemic organs, especially the brain
- Most common (50-75%) in posterior lung bases
- About 36% of AVMs are multiple and 50% bilateral
- Hepatic involvement
- Found in 8-31% of patients with OWRD
- May cause right upper quadrant pain
- Hepatomegaly
- Jaundice
- Symptoms of high-output cardiac failure are most common with large hepatic AVMs
- From large left-to-right shunt between hepatic arteries and veins and between portal vein and hepatic vein
- Bleeding from esophageal varices
- May be a cause of atypical cirrhosis
- Treatment
- Skin grafts to replace the nasal mucosa can reduce the incidence of epistaxis
- Embolization or ligation may be used on pulmonary or intrahepatic AVMs
- GI hemorrhage may require resection of the affected bowel
- Prognosis
- Excellent if bleeding is controlled

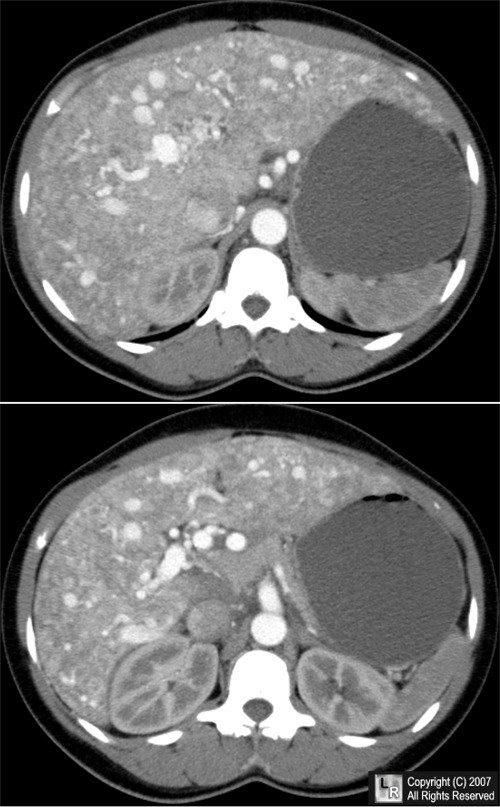
Osler-Weber-Rendu Disease. These two contrast-enhanced, axial CT scans
of the upper abdomen show multiple AVMs
(red arrows) in an enlarged liver
also containing numerous dilated blood vessels. The stomach is fluid-filled.
For this same photo without the arrows, click here.
For more information, click on the link if you see this icon 
For this same photo without the annotations, click here
Osler-Weber-Rendu Disease eMedicine Perry A Soriano, MD with James Petros, MD and James F McKinsey, MD, FACS
Osler-Weber-Rendu Disease National Center for Biotechnology Information Victor McKusick, MD Johns Hopkins University
|
|
|

{kind=link}
{kind=link}