|
|
Congenital Cystic Adenomatoid Malformation
CCAM
General Considerations
- Developmental hamartomatous abnormality with cyst production
- 25% of all congenital lung lesions
- Communicate with the tracheobronchial tree
- Usually receives blood supply from pulmonary circulation and drains to pulmonary circulation
- Types II and II may be associated with extralobar sequestration and receive systemic supply
Clinical Findings
- Most patients present in first month of life (70%) but sometimes discovered later in life because of recurrent pulmonary infections
- Usually present with respiratory distress
Imaging Findings
- The diagnosis can usually be made with conventional radiographs of the chest
- Equal predilection for each lung, slightly more common in upper lobes
- Lobar involvement is most common
- Prenatal ultrasound is accurate in diagnosing the disease usually at a mean gestational age of 22.6 weeks
- Early in life, the disease may present as a homogeneous, fluid-density mass because of delayed emptying of alveolar fluid, progressing to an air-filled cystic structure containing multiple air-fluid levels in cysts of varying size
- Although multiple cysts may be present, it may appear as one large cyst initially
- Shift of the mediastinum away from the lesion
- There is air-trapping in the cysts which may lead to rapid enlargement
- The most frequent finding on CT are small cysts (<2cm) associated with larger cysts or consolidated lung
Types of CCAM |
Type |
Description |
I |
Most common; composed of 1 or more cysts measuring 2-10 cm in size, larger cysts often associated with smaller cysts; walls contain muscle, elastic, or fibrous tissue. Cyst walls occasionally produce mucin which is unique to this subtype. |
II |
Small cysts (0.5-2 cm) of relatively uniform size resembling bronchioles; lined by cuboid-to-columnar epithelium with a thin fibromuscular wall. |
III |
Microscopic, adenomatoid cysts which are grossly a solid mass without clear cyst formation. |
Differential Diagnosis
- Congenital lobar emphysema
- Typically overexpansion of one lobe, most often an upper lobe
- Sequestration
- May look identical to CCAM if infected with air-fluid levels
- Bronchogenic cysts
- Well-circumscribed and fluid-filled
Treatment
- Surgical resection of the involved lobe in symptomatic patients
Complications
- May be associated with other congenital abnormalities up to 25% of time
- More common with Type II lesions and include renal, intestinal, cardiac and osseous abnormalities
Prognosis
- Depends on size of lesion
- Larger lesions are associated with vascular compromise, pulmonary hypoplasia and poorer prognosis
- Type III lesions are larger and have poorer prognosis


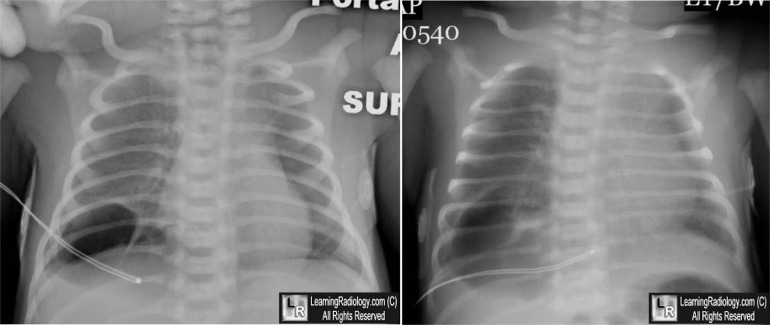
Congenital cystic adenomatoid malformation (CCAM). Chest radiographs obtained on day 2 and 3 of life show an expanding, air-filled cystic lesion (white and yellow arrows) in the right lower lobe. The newborn also had hyaline membrane disease. A Ct scan of the same child shows a cystic lesion in the right lower lobe with septations (green arrow) and an air-fluid level (blue arrow).
For more information, click on the link if you see this icon 
For these same photos without the annotations, click here and here
Congenital Cystic Adenomatoid Malformation. Gerald Mandell, MD. eMedicine
|
|
|

{kind=link}
{kind=link}