|
|
Scleroderma of the Lungs
Progressive Systemic Sclerosis
General Considerations
- Multisystem collagen vascular connective tissue disease mediated by a vasculitis
- Unknown etiology
- Most common form 30-50
- Female to male ratio of 3:1
- Pulmonary manifestations in 10-25% of patients with scleroderma, but…
- Lungs are involved in almost 100% of cases at autopsy
Clinical Findings
- Mildly productive cough
- Progressive dyspnea
- Hematemesis
- Pulmonary function abnormalities out of proportion to radiographs
Imaging Findings
- High resolution CT (HRCT) is best imaging study
- Chest radiographs can be insensitive to the presence of pulmonary disease and show abnormalities in only about 2/3 of patients with lung involvement
- Most prominent at lung bases bilaterally
- Interstitial disease which is primarily reticular
- Subpleural fibrocystic spaces (honeycombing)
- Low lung volumes from progressive volume loss
- Aspiration of refluxed gastric contents from disturbed esophageal motility
- Associated esophageal dilatation
- HRCT findings
- Pulmonary fibrosis and hypertension are most frequent findings
- Subpleural linear opacities with a basal distribution
- Subpleural cysts (honeycombing favors UIP)
- Irregular reticular opacities
- Septal thickening
- Traction bronchiectasis
- Thickening of the visceral pleural
- Micronodules
- Pleural disease including effusion is very uncommon in scleroderma
Differential Diagnosis
- Idiopathic pulmonary fibrosis
- Asbestosis
- Rheumatoid lung
Complications
- May be associated with systemic lupus erythematosis and dermatomyositis
- Pulmonary arterial hypertension
- Slightly increased incidence of lung cancer
- Sclerosis of cardiac muscle may contribute to cor pulmonale
Prognosis
- Overall: 50-67% 10-year survival rate
- Lung disease is leading cause of death from scleroderma
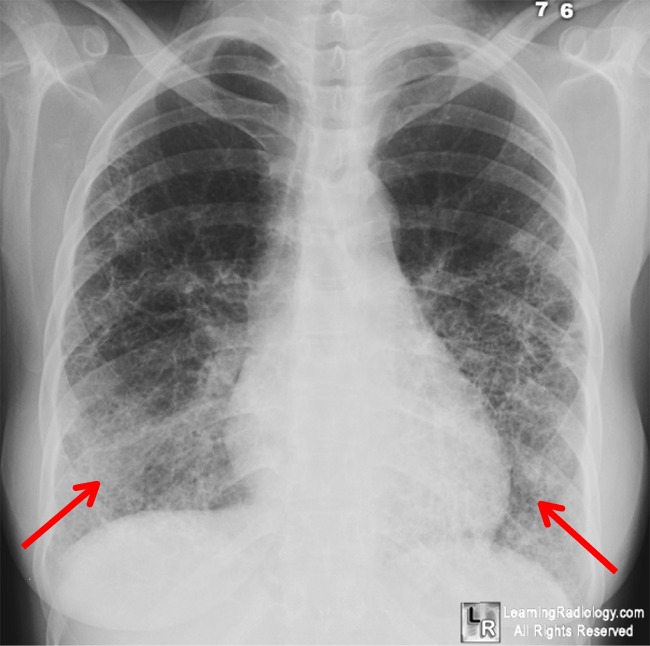
Scleroderma. Chest radiograph demonstrates coarse bibasilar reticular interstitial disease (red arrows).
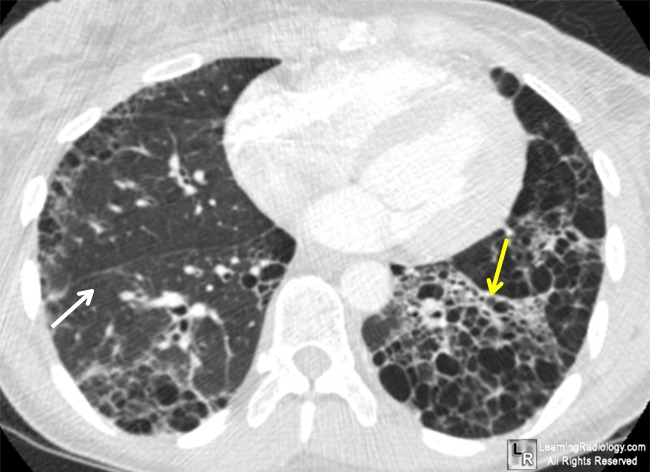
The axial CT scan shows linear opacities
(yellow arrow), subpleural cysts, ground-glass opacities (white arrow)
and thickening of the interlobular septae, primarily at the lung base in this patient.
For more information, click on the link if you see this icon 
For these same photos without the arrows, click here and here
Dahnert 5th ed
eMedicine Thoracic Scleroderma Elliot, T.
|
|
|

{kind=link}
{kind=link}