|
|
Tuberculous Empyema
General Considerations
- Represents a chronic, active infection of the pleural space
- The empyema contains many tubercle bacilli
- Empyemas are rare compared to reactive effusions in TB
- They result from numerous organisms spilling into pleural space
- Usually from rupture of a cavity, or
- Incidence of empyemas was historically higher in the pre-anti-tuberculous agent period when treatments for TB included therapeutic pneumothoraces, oleothorax, ping-pong ball plombage, pneumonectomy or thoracoplasty

Clinical Findings
- Frequently asymptomatic and found on routine surveillance, or when patient develops either:
- Pleural fluid in the empyema is thick and usually grossly purulent
- Smear is positive for acid-fast bacilli
- May TB empyemas contain cholesterol causing the mistaken gross impression that they are composed of chyle
Imaging Findings
- Thickened pleural rind, frequently calcified
- Almost always unilateral
- May have an associated extrapleural mass (empyema necessitatis)
- A collection of inflammatory tissue that spontaneously ruptures through a weakness in the chest wall into surrounding soft tissues.
- Can be caused by many infectious agents but mycobacteria are most common cause
- Usually associated with some evidence of parenchymal TB
- Tuberculous empyema is suspected on CT when there is a thick, calcific pleural rind, especially if there is associated rib thickening adjacent to the loculated pleural fluid
Differential Diagnosis
Treatment
- Therapy is usually via surgery using
- Parietal decortication, thoracoplasty, with or without omentopexy/myoplasty
- Antituberculous drug therapy is mandatory to sterilize all residual TB
Complications
- Bronchopleural fistula
- Empyema necessitatis
- Inability to re-expand the trapped lung and difficulty in achieving therapeutic drug levels in pleural fluid

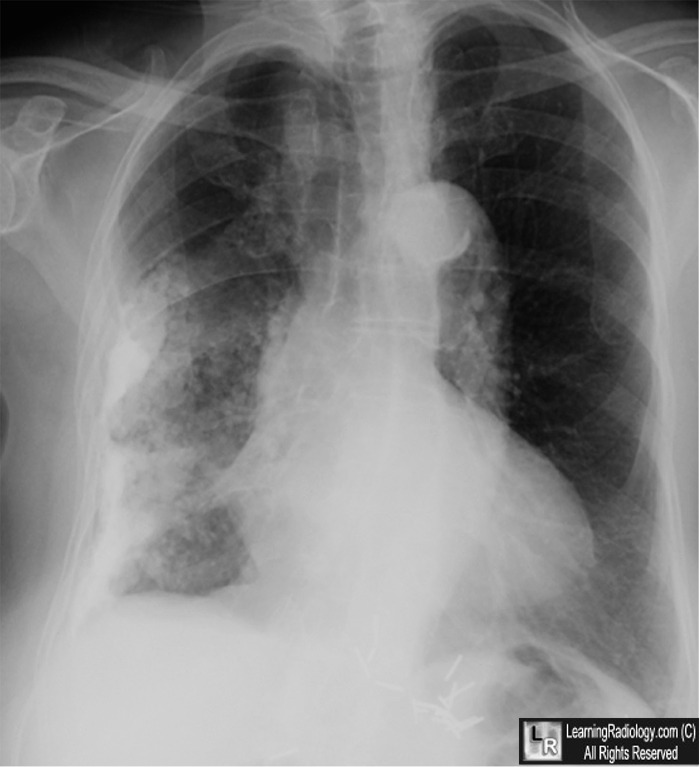
Tuberculous Empyema. A frontal radiograph of the chest demonstrates a thick and irregular rind of calcified pleura (yellow arrows) in the right hemithorax with slight shift of the heart and mediastinal structures towards the right due to volume loss. The left hemithorax shows no pleural calcification. This is a typical presentation of a calcified tuberculous empyema.
For this same photo with the arrows, click here
For more information, click on the link if you see this icon 
Southern Medical Journal Jover, F; Andreu, L; Cuadrado, J; Montagud, J: and Merino,J Tuberculosis Empyema Necessitatis in a Man Infected With the Human Immunodeficiency Virus 95(7):751-755, 2002
Seminars of Respiratory Infection Sahn, SA and Iseman, MD Tuberculous Empyema 1999 Mar;14(1):82-7
|
|
|

{kind=link}