|
|
Right Middle Lobe Atelectasis
General Considerations
- All types of atelectasis involve loss of volume in some or all of a lung with resultant increased density of the involved lung
- The atelectasis referred to here is that caused by bronchial obstruction, usually a tumor (i.e. a bronchogenic carcinoma), a foreign body or a mucus plug
- In asthmatics, chronic inflammation along with thicker and more viscous mucous leads to plugging and impaction of the bronchi
Signs of atelectasis -- general
- Increase in density of the affected lung
- Displacement of the fissures or the mediastinum towards the atelectasis
- Crowding of the vessels and bronchial tree in the area of volume loss
- Elevation of the hemidiaphragm
- Overaeration of the opposite lung
Right Middle Lobe Atelectasis
- Right middle lobe is more prone to atelectasis because its bronchus has a narrow diameter, acute angle of take-off and a relatively long course
- Causes of right middle lobe atelectasis include
- Asthma
- Cystic fibrosis
- Bronchopulmonary dysplasia
- Foreign body aspiration in the airway
- Tumors
- Primary endobronchial (i.e. bronchogenic carcinoma)
- Extrinsic compression from adenopathy
- Granulation tissue, as in TB
- Bronchopneumonia
- Imaging findings
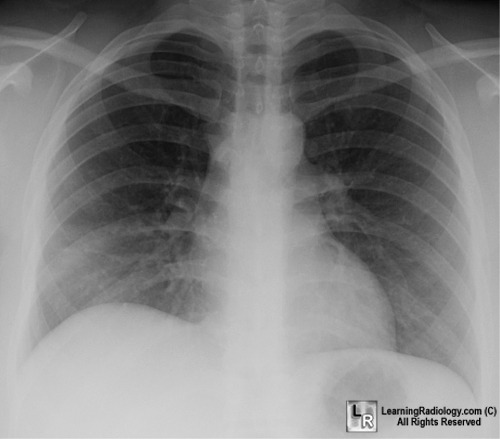
- Right middle lobe atelectasis is usually easier to recognize on the lateral view than the frontal view, where it may produce very subtle findings
- Silhouetting of the right heart border on the frontal view by the adjacent un-aerated medial segment of the middle lobe
- If the atelectatic middle lobe swings upward and anteriorly, it may produce a wedge-shaped density on the frontal view with its base at the heart

- Depression of the minor fissure and elevation of the major fissure, especially well seen on the lateral view
- On the lateral view, the atelectatic lobe forms a triangular density with its apex at the hilum and its base more peripheral in the lung
- If there is a nodular density seen at the apex of the triangle on the lateral view, suspect a mass in the hilum producing the atelectasis
- Elevation of the right hemidiaphragm may occur
- Treatment
- Chest physical therapy
- Bronchoscopy
Right Middle Lobe Syndrome
- Frequently occurs in children, with asthma a relatively common etiology
- Mainly based on chronic or recurrent right middle lobe atelectasis, rather than acute etiology
- Some authors believe the loss of volume is a primary inflammatory condition of the middle lobe aided by its isolation from the upper and lower lobe rather than caused by obstruction
 
Right Middle Lobe Atelectasis. Frontal radiograph of the chest (left) demonstrates indistinctness of the right heart border (white arrow) and slight elevation of the right hemidiaphragm from volume loss. The lateral view of the chest (right) shows downward displacement of the minor fissure (red arrow) and slight upward bowing of the major fissure (black arrow), both bordering the increased triangular density of the atelectatic middle lobe.
For additional information about this disease, click on this icon if seen above.
For same photos without annotations, click here or here
Fraser and Pare
|
|
|

){kind=link}
{kind=link}
{kind=link}