|
|
Five Common Causes of Neonatal Lung Disease
Transient tachypnea of the Newborn
Hyaline Membrane Disease
General Considerations
- Lack of sufficient surfactant production
- pressure to keep alveoli open; ¯ lung compliance
- Predisposed
- Premature infants < 34 weeks
- Cesarean-section
- Infants of diabetic mothers
- ¯ Lecithin/sphingomyelin ratio in amniotic fluid
- Thin rim of fibrin coats terminal bronchioles and alveolar ducts
- Result of, rather than cause of, this disease
- Other diseases produce hyaline membranes
- Meconium aspiration and BPD
- Hence, it is also called Respiratory Distress Syndrome of the Newborn
Clinical Findings
- Symptoms present in first 2 hours of life
- Symptoms that begin > 8 hrs are not due to HMD
- May in severity from 24 - 48 hours
- Then, gradual improvement > 48-72 hours
Imaging Findings
- Typically, diffuse “ground-glass” or finely granular appearance
- Bilateral and symmetrical distribution
- Air bronchograms are common
- Especially extending peripherally
- Hypoaeration in non-ventilated lungs
- Hyperinflation excludes HMD
- “Granularity” is the interplay of
- Air-distended bronchioles & ducts
- Background of atelectasis of alveoli
- May change from film-to-film if there is
- Expiration (air disappears)
- Better aeration (small bubble formation)
Treatment
- Positive end-expiratory pressure (PEEP
- Continuous positive airway pressure (CPAP)
- Surfactant administered via ETT
- Oxygen and diuretics
Prognosis
- In the past, almost all infants died of HMD by 72 hrs
- With assisted ventilation, recovery >90%
- All that follows represent complications of treatment, rather than of the disease
Complications
Pulmonary Interstitial Emphysema (PIE)
- Usually occurs on day 2 or 3
- Earlier it occurs, more ominous the sign
- Air is in lymphatics
- Small bubbles, streaky appearance of air
- Frequent precursor to PTX
Worsening Opacification
- Congestive heart failure (from PDA or fluid overload)
- Persistent patency of ductus arteriosus
- Oxygen stimulus is missing to close ductus
- Worsening pattern of RDS itself
- Development of BPD
- Superimposed pneumonia (uncommon)
- Pulmonary hemorrhage (uncommon)
Chronic Complications
- Lobar emphysema
- Localized interstitial emphysema
- Recurrent respiratory tract infections
- Retrolental fibroplasia
- Subglottic stenosis from intubation
Bronchopulmonary Dysplasia (AKA Chronic Respiratory Insufficiency of the Premature)
General Considerations
- BPD is consequence of early acute lung disease
- BPD may complicate HMD
- Also meconium aspiration syndrome and pneumonia
- Common to most is oxygen administered under positive pressure
- One definition involves an oxygen requirement at 28 days of life to maintain arterial oxygen tensions >50 mm Hg accompanied by abnormal chest radiographs
- Rarely occurs in infants > 1250 g and in infants born after 30 weeks gestation
Imaging Findings
- May be impossible to distinguish early stages of BPD from later stages of HMD
- Coarse, irregular, rope-like, linear densities
- Represents atelectasis or fibrosis
- Lucent, cyst-like foci
- Hyperexpanded areas of air-trapping
- Hyperaeration of the lungs
- Conglomerate disease in BPD
- Shifting atelectasis
- Episodes of aspiration or pulmonary edema
- Superimposed pneumonia
- Changes of BPD will revert to normal on the chest radiograph in most patients after the age of two
Differential Diagnosis
- Pulmonary interstitial emphysema (PIE) may look identical
- Smaller air-containing spaces in PIE (bubbly appearance)
- Meconium aspiration may look identical
- But history is different (BPD=preemie with chronic dz)
- Shunts
- Such as a patent ductus arteriosus
- Infection
- Especially with group A beta streptococci
- Congestive heart failure and pulmonary edema
Complications
- Sudden infant death
- Pulmonary arterial hypertension
- Increased risk of pulmonary infection
- Development of asthma
Transient Tachypnea of the Newborn (TTN)
General Considerations
- Usually full-term or slightly preterm
- Some delivered by C-section; some precipitous labor
- Mild respiratory distress immediately after birth
- Improve within several hours
Imaging Findings
- Hyperinflation of the lungs
- Fluid in the fissures
- Laminar effusions
- Fuzzy vessels
Treatment
- Oxygen
- Maintenance of body temperature
- Improvement most often occurs in < 24 hrs
Differential Diagnosis of TTN
- CHF
- TTN appears earlier and clears within < 24 hrs
- Neonatal pneumonia
- Infant with TTN not as sick; TTN clears rapidly
- Meconium aspiration syndrome
- Infant with TTN is term and not meconium stained
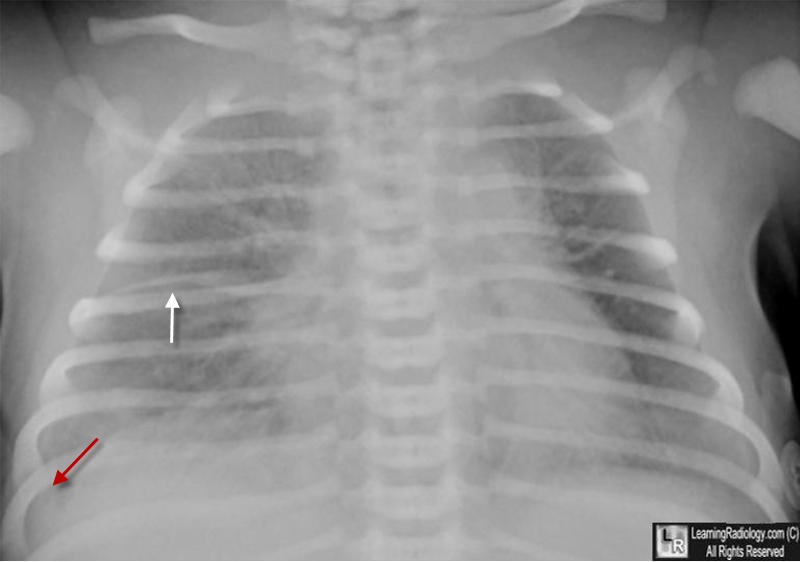
Transient Tachypnea of the Newborn (TTN). Frontal radiograph of the chest of a term newborn shows streaky, perihilar linear densities, indistinctness of the blood vessels and fluid in the minor fissure (white arrow) along with a small right effusion (red arrow), all signs of increased fluid in the lungs.
Meconium Aspiration Syndrome
General Considerations
- Most common cause of neonatal respiratory distress in full-term/postmature infants
- Hyaline membrane disease most common cause in premature infants
- Pathogenesis
- Meconium in amniotic fluid of 20% of pregnancies
- Meconium products produce bronchial obstruction and air-trapping
- Chemical pneumonitis
Clinical Findings
- Post-mature
- Severe respiratory distress almost immediately
- Respiratory distress more severe than TTN
Imaging Findings
- Diffuse “ropey” densities (similar to BPD)
- Patchy areas of atelectasis and emphysema from air-trapping
- Hyperinflation of lungs
- Spontaneous pneumothorax and pneumomediastinum
- Occurs in 25%; usually requiring no therapy
- Small pleural effusions (20%)
- No air bronchograms
- Clearing usually quick if mostly water; days-weeks if mostly meconium
Treatment
- Supportive
- Antibiotics and oxygen
- ECMO can be used
- Complications
- Pulmonary hypertension → R→L shunting
- Cyanosis
- Anoxic brain damage
Neonatal Pneumonia
General Considerations
- Etiology
- Intrauterine infection or during delivery
- Most are bacterial in origin
- Group A Beta nonhemolytic Strep used to be most common
- Now E. Coli in preemies
Clinical Findings
- Not febrile
- Marked respiratory distress
- Tachypnea
- Metabolic acidosis
- Septicemia and shock
Imaging Findings
- Perihilar streaky pattern may resemble TTN
- Patchy airspace disease
- Diffuse, relatively homogeneous infiltrates resembling ground-glass pattern of HMD
- Occasionally pleural effusion may occur
- Lobar consolidation from infection is unusual in a newborn
- Group B Strep looks most like HMD
- Term infant with findings of “HMD” should be considered to have pneumonia until proven otherwise
Treatment
- Appropriate antibiotic
- Oxygen
- Fluid support as needed
- Streptococcal Pneumonia
- Complications and Associations
- Complications
- Bronchiectasis
- Lung abscess
- Glomerulonephritis
- Associated with
- Delayed onset of diaphragmatic hernias in newborns
- Chlamydial Pneumonia
- Contamination during delivery
- Develops at 2 to 12 weeks of age
- Tachypneic but usually not critically ill
- Conjunctivitis caused by same organism
- X-rays show bilateral interstitial infiltrates
- Treatment with erythromycin → rapid resolution

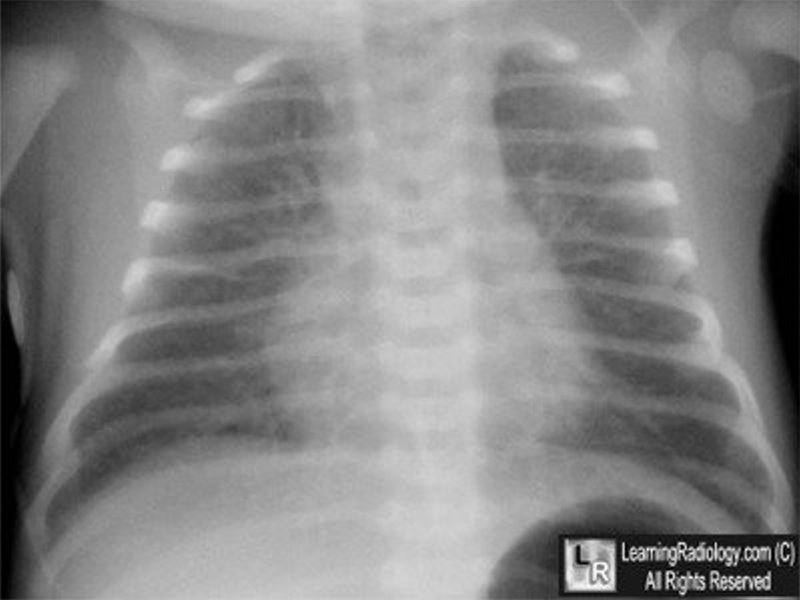
Transient Tachypnea of the Newborn (TTN). Frontal radiograph of the chest of a term newborn (left) shows streaky, perihilar linear densities (white circles), indistinctness of the blood vessels and fluid in the minor fissure (black arrow), all signs of increased fluid in the lungs. Three days later (right), a frontal radiograph of the same baby shows complete clearing of the fluid and a normal chest radiograph.
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
|
|
|

{kind=link}
{kind=link}