|
|
Bronchopulmonary Dysplasia
Chronic Lung Disease of Infancy
General Considerations
- First described as a chronic lung disease seen in premature newborns treated for respiratory distress syndrome (RDS) with supplemental oxygen and mechanical ventilation for at least one week
- It is now recognized that bronchopulmonary dysplasia (BPD) may complicate other types of neonatal lung disorders such as meconium aspiration syndrome and pneumonia
- Common to almost all causes is oxygen administered under positive pressure
- One definition involves an oxygen requirement at 28 days of life to maintain arterial oxygen tensions >50 mm Hg accompanied by abnormal chest radiographs
- Rarely occurs in infants > 1250 g and in infants born after 30 weeks gestation
- Most common in those with a birth weight of < 1000g, born at 22-32 weeks of gestation
- Incidence of bronchopulmonary dysplasia defined as a continued need for oxygen at 36 weeks (corrected age) is 30% for infants <1000g at birth
- Potentiating factors
- Pulmonary edema
- Infection
- Poor nutritional status
Clinical Findings
- Tachypnea and tachycardia
- Retractions
- Oxygen desaturation
- Weight loss
Imaging Findings
- It may be impossible to distinguish the early stages of bronchopulmonary dysplasia from the later stages of respiratory distress syndrome (hyaline membrane disease)
- Coarse, irregular, rope-like, linear densities
- Represents atelectasis or fibrosis
- Lucent, cyst-like foci
- Hyperexpanded areas of air-trapping
- Hyperaeration of the lungs
- Shifting atelectasis
- Episodes of aspiration or pulmonary edema
- Superimposed pneumonia
- Changes of bronchopulmonary dysplasia will revert to normal on the chest radiograph in most patients after the age of two
Differential Diagnosis
- Pulmonary interstitial emphysema (PIE) may look identical
- Smaller air-containing spaces in PIE (bubbly appearance)
- Left-to-right shunt such as a patent ductus arteriosus
- Infection, especially with non group A beta streptococci
- Congestive heart failure and pulmonary edema
Treatment
- Prevention of hypoxemia and anemia
- Diuretics
- Systemic corticosteroids
- Optimal nutrition
Complications
- Sudden infant death
- May go on to develop pulmonary arterial hypertension
- Increased risk of pulmonary infection
- Development of asthma
Prognosis
- With the use of surfactant replacement and antenatal steroids, survival has improved
- Main determinant of chronic morbidity is development of obstructive airway disease
- Demonstrated by a decreased forced expiratory flow (FEF)
- Increased airway reactivity
- Increased residual volume with a normal total lung capacity

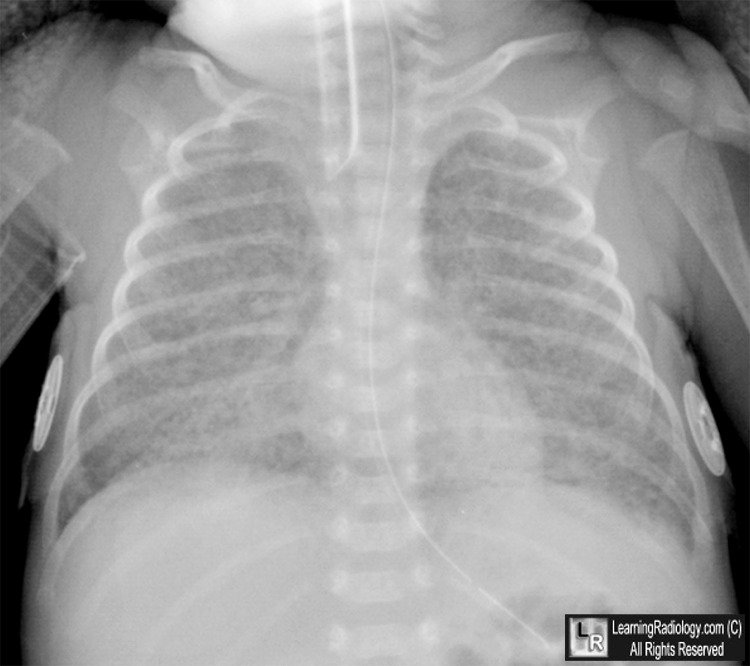
Bronchopulmonary Dysplasia. The lungs are usually overaerated. There are diffuse rope-like densities separated in some areas by zones of hyperlucency. The densities may be coalescent in many areas. The heart borders can be completely obliterated.
For this same photo, click here
For more information, click on the link if you see this icon 
Radiologic Clinics of North America Wood, B. The Newborn Chest 31:2 May 1993
Radiology of the Pediatric Chest Felman, A. McGraw-Hill 1987
Bronchopulmonary dysplasia eMedicine Driscoll, W and Davis, J
Am. J. Respir. Crit. Care Med., Volume 163, Number 7, June 2001, 1723-1729 Bronchopulmonary dysplasia Jobe, A and Bancalari, E
|
|
|

{kind=link}