|
|
Ewing Sarcoma
Submitted by Christina Kang, MSIV
General Considerations
- Second most common malignant bone tumor in children (after osteosarcoma)
- Accounts for approximately one-third of all primary bone tumors
- More common in males than females
- More common in Caucasians
- Occurs between the ages of 5-30 years
- Highest frequency between 5-15 years
- Location
- Arise in medullary cavity, usually of long bones in the lower extremities
- Most commonly occurs in long bones and pelvis
- Most occur in femur, pelvis, tibia, and humerus
- But they can occur in virtually any bone
- Commonly involves metadiaphysis of long bones
Clinical Findings
- Most common symptoms are localized pain and swelling
- Additional symptoms may include
- Weight loss
- Anemia
- Leukocytosis
- Elevated erythrocyte sedimentation rate
Imaging Findings
- Most lesions are visible on conventional radiographs
- However, their degree of spread is better evaluated with MRI
- Common manifestations on conventional radiography include
- Poorly marginated, lytic, destructive lesion
- Soft tissue mass or infiltration is common
- Soft tissue mass may occur without destruction of cortex
- Soft tissue mass may produce saucerization (scalloped depression in cortex)
- Periosteal reaction
 is common is common
- Lamellated - onion-skinning due to successive layers of periosteal development
- Sunburst or spiculated - hair-on-end appearance when new bone is laid down perpendicular to cortex along Sharpey’s fibers
- Codman’s triangle - formed between elevated periosteum with central destruction of cortex
- Osteosclerosis may be present secondary to reactive bone formation
- Other, less common, manifestations
- Thickened cortex
- Expansion of bone
- Pathologic fractures
- Radioisotope Bone Scan
- Increased uptake in areas of bone destruction
- Whole-body bone scans are used to detect metastatic lesions
- Metastases may be present in up to 30% of cases at time of diagnosis
- CT
- To evaluate bone destruction and extra-osseous involvement
- MRI
- Method of choice for tumor staging
- Assesses soft tissue involvement
- Low signal intensity on T1WI
- Heterogeneous gadolinium enhancement
- High signal intensity on T2WI
- Evaluates response to chemotherapy and radiation treatment
Differential Diagnosis
- Ewing sarcoma is one of the small, round cell lesions of bone, including
- Age and skeletal location may be important factors in narrowing the differential diagnosis
- Osteomyelitis
- Shorter duration of pain and less aggressive periosteal reaction than Ewing’s
- Eosinophilic granuloma
- Benign bone lesion with solid periosteal reaction
- Osteosarcoma
- Commonly occurs in long bones of young patients
- Homogeneous, cloudlike osteoid deposition in soft tissues
- Lymphoma
- Older age range
- Clinically healthy
Prognosis
- 60-75% five-year survival
- Predictors of poorer prognosis
- Non-resectable lesions, such as those in the pelvis
- Older age
- Elevated leukocyte count and sedimentation rate at presentation
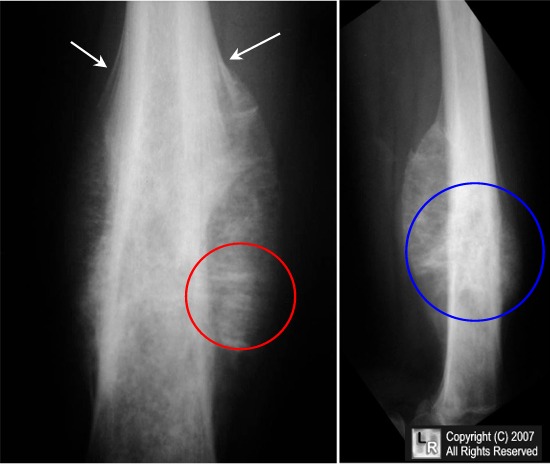
Ewing sarcoma of femur. Frontal radiograph and lateral radiographs of the femur
demonstrate mottled, osteolytic lesion (blue circle) with poorly marginated edges in the diaphysis of the bone.
There is sunburst periosteal reaction (red circle) and lamellated periosteal reaction (white arrows).
For additional information about this disease, click on this icon if seen above.
For this same photo without arrows, click here
eMedicine Ludwig G. Strauss, MD
Resnick 4th edition
Radiologic Clinics of North America Vol.31, No. 2, March 1993 Eggli, K., Quiogue, T. and Moser, R.
|
|
|

{kind=link}