|
|
Ureteral Calculus
General considerations
- About 12% of general population will develop a renal calculus by age 70
- Many will have an underlying metabolic disorder
- About 2-3% of general population will experience an attack of ureteral colic
- Much more common in males
- Peak onset in 3rd decade
- Type of stones
- Calcium oxalate 75%
- Struvite 15%
- Uric acid 5%
- Calcium phosphate 5%
- Cystine 1%
- Metabolic disorders that predispose to stone formation
- Hypercalcuria
- Such as might occur in hyperparathyroidism, milk-alkali syndrome, hypervitaminosis D, neoplastic disorders, sarcoidosis, Cushing’s syndrome
- Normocalcemia
- Such as might occur with obstruction, urinary tract infection, vesical diverticulum, horseshoe kidney, medullary sponge kidney, prolonged immobilization, renal tubular acidosis, idiopathic hypercalcuria
- Hyperoxaluria
- Hyperuricosuria
- Stones form in acidic urine
- Cystinuria
- Stones form in acidic urine
- Xanthinuria
- Urinary tract infection
- With alkaline urine, may lead to magnesium ammonium phosphate or struvite stones
- Nephrocalcinosis
Acute Obstruction By Ureteric Calculi
- Clinical findings
- Renal colic is characterized by acute colicky flank pain frequently radiating into pelvis, groin or testis
- Hematuria
- Most stones are impacted at narrowest points of ureter
- Ureteropelvic junction
- Iliac vessel crossing
- Ureterovesical junction
- Imaging findings
- Conventional radiography
- 60% of calcifications along expected course of ureter on symptomatic side are ureteric stones
- Stones may be present in 30% of the time when KUB is negative
- Intravenous pyelograms have largely been replaced by CT “stone searches”
- Ultrasound
- Unilateral pelvicaliectasis (up to 10% false-positive rate)
- Resistive index >0.7 in symptomatic kidney
- Absent ureteral jet on affected side (may be present with partially obstructing calculus)
- Direct visualization of prevesical calculus by transabdominal, transrectal, transvaginal US
- CT
- Highly sensitive, specific and accurate
- Study of choice is non-enhanced abdominal and pelvic CT= “stone search” protocol
- All stone compositions readily detectable
- Calculus within ureter
- Ureteric rim sign (77%) = ureteric edema surrounding impacted small ureteric calculus
- Ureterovesical junction edema
- Stranding of perinephric / paraureteric fat
- Perinephric fluid collection
- Renal enlargement
- Treatment
- Hydration maintaining urine output of 2-3 l/day
- Diet
- Restrict amounts of protein, sodium, calcium
- Drugs
- Pain medication
- Thiazide diuretics (lowers urinary calcium)
- Allopurinol (lowers urate and oxalate excretion)
- Prognosis
- Spontaneous passage of ureteral calculi in 93%
- Most stones <5 mm will eventually pass
- Without treatment, stone recurrence is 10% at 1 year, 33% at 5 years, 50% at 10 years
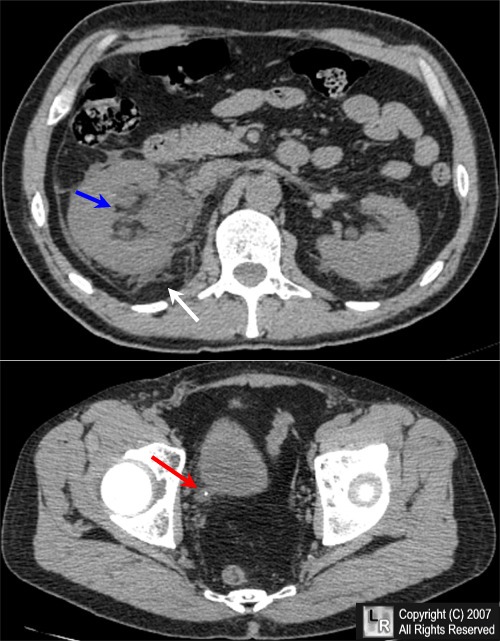
Obstructing Ureteral Calculus. Non-enhanced axial CT scan images of the abdomen and pelvis
demonstrate an enlarged right kidney with perinephric stranding (white arrow), a dilated intrarenal collecting system (blue arrow) and a calcific density at the ureterovesical junction (red arrow) with dilatation of the ureter.
For additional information about this disease, click on this icon above.
For this same photo without the arrows, click here
|
|
|

){kind=link}
{kind=link}