|
|
Fracture of the Dens
Odontoid Process Fracture
- General considerations
- Most dens fractures are caused by motor vehicle accidents and falls
- About 1/3 of C-spine injuries occur at C2 and about ½ at C6-C7
- As expected, most fatal cervical spine injuries occur at C1 or C2
- Most odontoid fractures occur with flexion, extension and rotation
- Normal anatomy
- Odontoid process (dens) of C2 (axis) articulates with C1 (atlas) with three joints
- Central atlantoaxial joint
- Bilateral. Lateral atlantoaxial joints
- Ligaments (transverse and dentate) provide rotational and translational stability
- Transverse ligament holds dens in close approximation to anterior arch of C1
- Dens represents the fused remnants of the body of C1
- Fractures of the dens
- About 15% of all cervical spine fractures
- Classified by location (Anderson and D’Alonzo classification)
- Type I (<5%)
- Tip of dens at insertion of alar ligament which connects dens to occiput
- Usually stable but may be associated with atlanto-occipital dislocation
- Type II (>60%)
- Most common dens fractures
- Fracture at base of dens at its attachment to body of C2
- Type III (30%)
- Subdentate—through body of C2
- Does not actually involve dens
- Unstable fracture as the atlas and occiput can now move together as a unit
- Other fractures include a rare longitudinal fracture through dens and body of C2
- Clinical findings
- Pain
- Inability to move ranging to quadriplegia
- Feeling of instability of head on spine
- There have been studies to examine the need for c-spine imaging in low risk patients. The Canadian criteria (table below) have been reported to be 99.4% sensitive in excluding significant cervical spine pathology
Canadian C-Spine Rules for Clearing
Low-Risk Patients of C-spine Injury |
Patient must be alert (GCS 15) |
Not intoxicated |
No “distracting” injury (e.g. no fracture of long bone or large laceration) |
Low risk (i.e. not older than 65 or had a dangerous mechanism of injury, paresthesias in extremities) |
Low risk factors such as rear-end collisions, ambulation at any time post-trauma, delayed onset of neck pain, absence of midline cervical tenderness, can maintain seated position in ED) |
Patient can actively rotate head 45 degrees right or left |
- Imaging findings
- Conventional radiography is frequently first used as it tends to be most available
- CT is better at demonstrating fractures
- MRI is used for evaluation of ligamentous, disk, spinal cord and soft tissue injuries
- Posterior displacement of the fractured dens into the spinal canal is more common than other displacements
- Lateral view on conventional radiography is most useful as most (85-90%) of injuries can be seen on lateral view
- Cervicothoracic junction visibility assures that the entire cervical spine is visualized
- Soft tissue findings may include >5 mm of prevertebral soft tissue at C3 or less than half of the AP diameter of the adjacent vertebra
- At level of C6, prevertebral soft tissue should be no more than 22 mm in adults and 14 mm in children younger than 15 years
- Widening of the predentate space to greater than 3 mm is abnormal
- Pitfalls
- A mach line may appear to traverse the base of the dens on the open-mouth (aka as the atlantoaxial or odontoid) view but should be recognized by the superimposed base of the occiput
- The mach line will not be present on the lateral view of the dens
- A smooth and sclerotic edge to the “fracture” usually indicates either congenital non-union or acquired non-union of the dens to the body of C2
- Treatment
- Type I fractures are usually treated with a hard collar for 6-8 weeks
- Type II fractures can be treated with
- Halo immobilization for 12-16 weeks
- Operative fixation (odontoid screw)
- Arthrodesis of C1 to C2
- Type II fractures can be treated with a halo or surgically, as Type II fractures
- Complications
- Non-union
- Due to limited vascular supply
- May occur in 30-50% of Type II fractures, especially in elderly
- Malunion
- Pseudarthrosis
- Affected by age of patient, amount of displacement
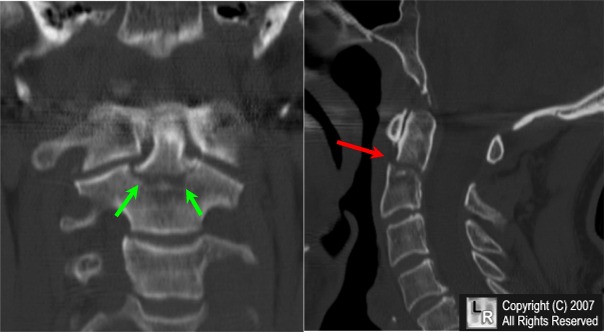
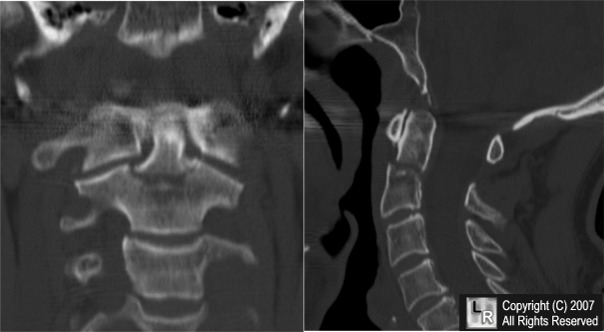
Fracture of the Dens. These are two reformatted CT images of the cervical spine. The green arrows point to a transverse
fracture of the base of the dens (odontoid) (Type II). The red arrow points to the same fracture of the sagittal reformatted image.
The dens is displaced slightly posteriorly on the body of C2.
For the same photo without the arrows, click here
|
|
|

){kind=link}
{kind=link}