|
|
Osteochondroma
General Considerations
- Osteochondroma is the most common benign bone tumor and the most common skeletal neoplasm
- They account for approximately 35% of all benign bone tumors and 9% of all bone tumors
- They are cartilage-capped bony projections from the external surface of a bone
- They occur only in bones which form by enchondral bone formation and most commonly found around the knee (40%) and shoulder, although they can occur in any bone
- Almost all are diagnosed in patients under the age of 20 with a marked male:female predominance (3:1)
- They grow until skeletal maturity and then stop growing when the epiphyseal plate fuses, although the cartilage cap can continue to grow slowly until about age 30
- Osteochondromas tend to occur near an epiphyseal growth plate and grow away from the physis
Clinical Findings
- Most are diagnosed incidentally
- Or, they may come to clinical attention because they produce a mass
- They are usually asymptomatic
- When painful, they should be evaluated for
- Mechanical irritation and inflammation of the surrounding soft tissues
- Fracture of the stalk
- Avascular necrosis of the cartilaginous cap
- Malignant degeneration
Imaging Findings
- Conventional radiography is the study of first choice
- CT can be used to determine if the marrow and cortices of the lesion are continuous with the parent bone
- MRI can be used to asses surrounding soft tissues and to measure the thickness of the cartilage cap, which can be important in evaluating for malignant generation
- A thick cartilaginous cap (>1 cm) in adults should raise the possibility of malignant transformation
- They can vary is size considerably, with the average tubular bone lesion being about 4 cm
- Osteochondromas can either be sessile (flat) or pedunculated (stalk)
- Sessile lesions are more likely to be associated with abnormalities of tubulation of the underlying bone leading to metaphyseal widening or a "trumpet shaped” deformity on x-ray
Malignant Degeneration
- Fewer than 1% of solitary osteochondromas undergo malignant degeneration of the cartilage cap into secondary chondrosarcoma
- It is usually preceded by
- New onset of growth of the lesion
- Rapid growth of a lesion, or
- New onset of pain
- The risk of malignant degeneration increases with an increase in the number and size of the osteochondromas
- In general, a sessile lesion is more likely to degenerate into sarcoma than a pedunculated lesion (exostosis)
Associations and Syndromes
- Hereditary multiple exostoses
- Autosomal dominant condition
- Short stature
- Multiple osteochondromas
- Asymmetric growth at the knees and ankles
- Risk of malignant degeneration is 1-20%
- Dysplasia epiphysealis hemimelica (DEH, Trevor disease)
- Osteochondromas arising in the epiphyses
- Involve the joint
- Lesions restricted to one side of the body–either left or right
- May be multiple lesions in a single limb
- Primarily involves one side of an epiphysis
- Medial side is affected twice as often as the lateral side
- Usually occurs in infants or young children
Treatment
- There is no treatment necessary for asymptomatic osteochondromas
- The cornerstone of treatment is observation because most lesions are asymptomatic
- If the lesion is causing pain or neurologic symptoms due to compression, it should be resected at the base
- None of the cartilage cap or perichondrium should be left in the resection bed or recurrence can occur.
- As long as the entire cartilage cap is removed there should be no recurrence
- Patients with many large osteochondromas should have regular radiographic screening exams for the early detection of malignant transformation

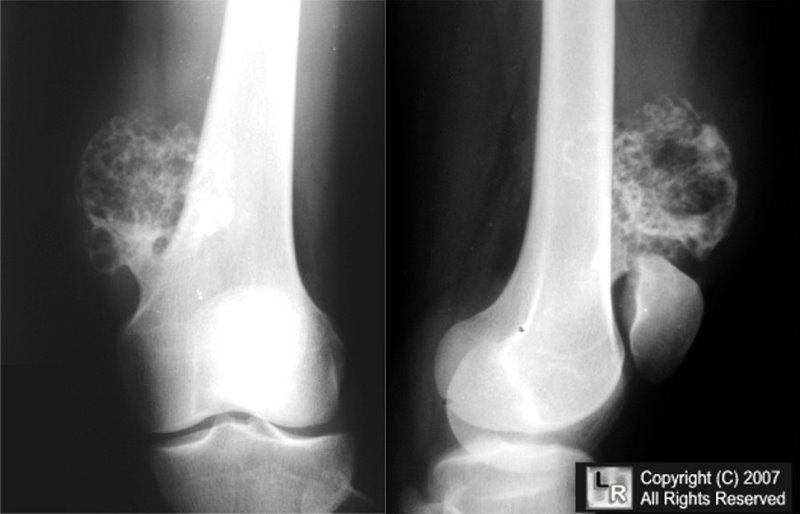
Osteochondroma. The white arrows point to a mushroom-shaped, pedunculated bony
excrescence arising from the anteromedial aspect of the distal femoral metaphysis, attached to the parent bone and
pointing away from the metaphysis.
For this same photo without the arrows, click here
For more information, click on the link if you see this icon 
Henry DeGroot III, MD
eMedicine Ian D Dickey, MD, FRCSC
|
|
|

{kind=link}