|
|
Pneumonia - Gram positive and Gram negative
Gram Positive Pneumonias
Pneumococcal pneumonia
- Most common gram positive pneumonia
- 90% community acquired
- Organism: strep pneumoniae
- Usually found in compromised hosts, elderly, debilitated
- Most often types 8, 4, 5 and 12
- Type 3 is especially fatal to elderly
- Sicklers are particularly prone to pneumococcal pneumonia
- Produces inflammatory edema in the alveoli which spreads via pores of Kohn to more lateral alveoli
Imaging
- Extensive infiltrate usually abutting pleural surface
- Prominent air bronchograms (DDX: Staph has no air bronchogram)
- Organism is aspirated into the lungs from the upper airways so it shows a predilection for lower lobes
- Does not respect segmental boundaries
- Resolution begins promptly with antibiotics – frequently within 24 hours
- DDX for alveolar infiltrates with clearing in 24 hours includes
- Hemorrhage into lungs,
- Pulmonary edema
- Pneumococcal pneumonia
- Aspiration
Staph aureus pneumonia
- Most common bronchopneumonia
- Overwhelming majority hospital-acquired
- Most common cause of death during influenza epidemics
- Rarely develops in healthy adults
- Hemolyzes blood agar
- Its ability to produce pathology in humans is due to its production of coagulase
- Produces its pathologic reaction in the conducting airways
Imaging
- Rapid spread through the lungs
- Empyema, especially in children
- No air bronchogram
- Pneumothorax
- Abscess formation
- Bronchopleural fistula
- In children
- Rapidly developing lobar/multilobar consolidation
- Pleural effusion (90%)
- Pneumatocoele
- In adults
- Patchy bronchopneumonia of segmental distribution, frequency bilateral
- May be associated with atelectasis since airways are filled (not so with pneumococcal)
- Pleural effusion (50%)
Streptococcus pyrogenes pneumonia
- Most common in winter
- Only 5% of bacterial pneumonias
- Group A Beta hemolytic strep
- Predisposed: Newborns and following measles
Imaging
- Looks like staph pneumonia but with less of a tendency to produce pneumatocoeles
- Almost always in the lower lobes
- Patchy bronchopneumonia
- Empyemas do form
- Complications:
- Bronchiectasis
- Lung abscess
- Glomerulonephritis
- Associated with delayed onset of diaphragmatic hernias in newborns
Gram Negative Pneumonias
Pseudomonas aeruginosa
- Gram negative rod
- Frequently hospital acquired
- Affects patients with COPD, CHF alcoholism, kidney disease, those with trachs
- Frequently related to use of inhalators or nebulizers
- Many patients are on multiple antibiotics and/or steroids
Imaging
- Resembles staph pneumonia
- Predilection for the lower lobes
- Usually affects both lungs
- Has multiple small lucencies within it
- Lung abscess greater than 2 cm may also occur
- Widespread nodular shadows is another manifestation
Klebsiella, Enterobacter, Serratia
- Encapsulated, gram negative rods
- Most are hospital acquired
- Most are chronic alcoholics
- Aspirated into lungs so most are unilateral and right sided
Imaging
- Produces excessive amounts of inflammatory exudate which cause the affected lung to gain volume and the fissures to bulge
- Abscess and cavity formation are common
- Pleural effusion and empyema are common
- May result in gangrene of the lung where massive pieces of lung tissue fall into an abscess cavity
- Serratia marcescens may cause bronchopneumonia
Anaerobic organisms
- Frequently from aspiration of gastric contents
- Organisms include Bacteroides melaninogenicus, B. fragilis
Imaging
- Almost always lower lobes
- Frequently right sided
- Homogeneous consolidation
- About 70% will have pleural involvement–effusion, empyema–which may progress very rapidly
- Half develop abscesses
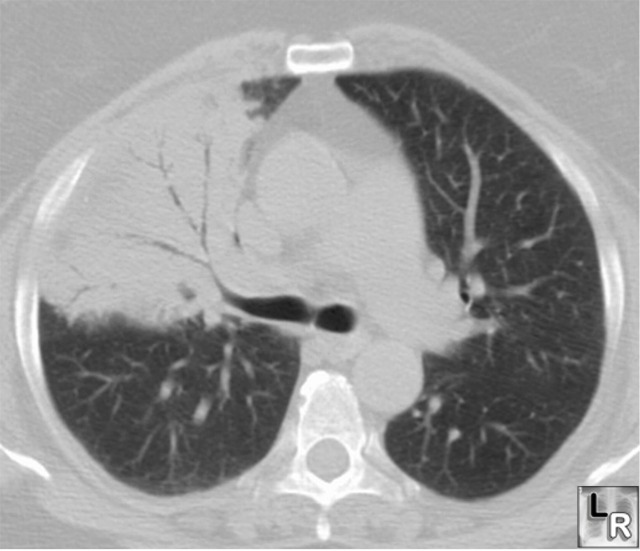
Pneumococcal
pneumonia produces
consolidation
in the
right
upper lobe
with
multiple
air
bronchograms
(black
branching
structures)
present
since the
spaces
surrounding
the
air-filled
bronchi
normally
contain
air but
now are
filled
with
inflammatory
exudate.
There is
no
cavitation,
the
disease is
in the
lower lobe
and it
contains
air
bronchograms,
all
characteristics
of
pneumonia
caused by
Streptococcus
Pneumoniae
(formerly
known as
Diplococcus
Pneumoniae)
|
|
|
