|
|
Pelvic Congestion Syndrome
Submitted by Yasmin Chaudhri, MD
-
Common cause of chronic pelvic pain
- Frequency
- Approximately 10% of the general female population may have pelvic varices, and 60% of those women may develop this syndrome
- Clinical Symptoms
- Chronic dull pelvic pain, pressure, and heaviness
- Often associated with movement, posture, and activities that increase abdominal pressure
- Unilateral or bilateral
- Often asymmetric
- Physical examination findings
- Varicose veins and ovarian point tenderness
- Pathophysiology
- Probably multifactorial and may include:
- Dilated and tortuous ovarian veins secondary to retrograde flow through incompetent valves
- Obstructing anatomic anomalies
- Retroaortic left renal vein
- Left ovarian vein congestion due to compression of the left renal vein by the superior mesenteric artery (nutcracker phenomenon)
- Right common iliac vein compression
- Secondary congestion can be seen in various disorders including:
- Valvular incompetence
- Portal hypertension
- Acquired inferior vena cava syndrome
- Risk Factors
- Hereditary factors
- Hormonal influence
- Pelvic surgery
- Retroverted uterus
- History of varicose veins
- Multiple pregnancies
- Imaging Findings
- Venography
- Direct visualization of dilated pelvic veins
- Transvaginal Ultrasound:
- Identification of multiple dilated structures around the uterus and ovaries with venous blood Doppler signal
- Dilated pelvic vein with a diameter greater than 4 mm
- Slow blood flow (about 3 cm/sec)
- Dilated arcuate vein in the myometrium communicating between bilateral pelvic varicose veins
- More than 50% of women have associated cystic ovaries
- MR Imaging:
- Dilated, tortuous, enhancing tubular structures near the uterus and ovary; may see extension to the broad ligament and pelvic sidewall
- T1-weighted images: varices appear as flow voids
- Gradient-echo MR: varices have high signal intensity
- T2-weighted images: usually varices appear low in signal intensity
- 3D T1 gradient-echo sequences with gadolinium: varices have high signal intensity
- Treatment
- Medical Treatment
- May be used for underlying disorders
- Procedural Treatments:
- Laparoscopic transperitoneal ligation of ovarian veins
- Percutaneous coil embolization of the gonadal vein
- Interventional stent placement for anatomic anomalies
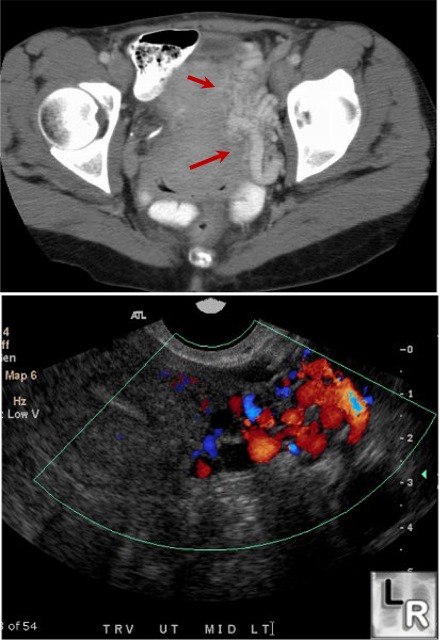
Pelvic Congestion Syndrome. CT (top)
and Color
Doppler
Ultrasound
(bottom) of
pelvis. CT of the
pelvis with
intravenous
contrast
shows
multiple,
dilated and
tortuous
pelvic veins
(red arrows)
near the
patient's
uterus on the
patient's left
side. Color
Doppler
ultrasound of
the same area
demonstrates
extensive
venous blood
Doppler signal
|
|
|
