|
|
Fibromuscular Dysplasia
Fibromuscular Hyperplasia, FMH
Submitted by Ab Shrivastava, MD
- General Considerations
- Incidence
- 0.6% via angiography
- 1.1% via autopsy
- Female to male ratio 3:1
- Presenting age 25-50
- Pathology
- Developmental lesion of unknown etiology which can affect multiple vessels.
- Consists of areas of heaped intima, adventitia, and media alternating with areas of medial destruction resulting in small focal aneurysms.
- 3 histologic types
- Intimal fibroplasia
- Medial fibroplasia, and
- Subadventitial (perimedial) fibroplasia of the arterial wall
- 3 subtypes not always apparent on imaging. Classic “string of beads” appearance on angiography for medial fibroplasias
- Some authors describe 5 total subtypes. Medial fibroplasias divided into medial fibroplasia with aneurysm and medial fibromuscular dysplasia. Perimedial fibroplasias subdivided into subadventitial and adventitial fibroplasias
- Medial fibroplasias most common
- Clinical Findings
- Renovascular hypertension (if bilateral renal arteries involved).
- Transient ischemic attack
- Intracranial aneurysm/thromboembolic stroke
- Often asymptomatic
- Location
- Renal arteries 85%
- Only 40% have bilateral renal artery involvement
- Most often middle and distal 1/3 of renal arteries involved
- Less commonly affected: Internal carotid (often bilateral), vertebral, mesenteric, celiac, hepatic, iliac arteries
- If FMD is found at any location, one must evaluate carotid arteries for lesions
- Imaging Findings
- Angiography considered gold standard. CTA and MRA becoming more sensitive.
- FMD is characterized by
- Narrowing of the affected vessel with a “string of beads” or nodular appearance , due to focal annular repetitive intimal and medial proliferative changes
- Differential Diagnosis
- Really a classic appearance
- Only entity on differential is atherosclerosis
- Treatment
- If symptomatic (intractable hypertension), improvement to renal blood flow can be me made via surgery or angioplasty
- Angioplasty is less invasive and cure rate is approximately 50% and improvement in 30% of patients
- Angioplasty suitable for noncalcified short segments
- Surgery reported to have lower re-stenosis rate and greater improvement in GFR
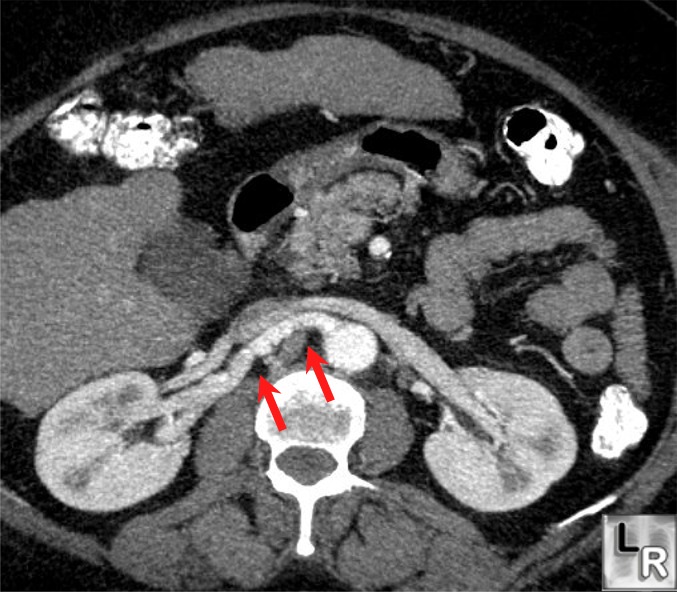
Fibromuscular Dysplasia. CT of
the abdomen with
IV contrast
demonstrates
nodularity
(string-of-beads
sign) of the
right renal
artery (arrows)
characteristic
of fibromuscular
dysplasia
(hyperplasia)
http://www.uhrad.com/ctarc/ct015.htm
http://www.emedicine.com/radio/topic280.htm
http://chorus.rad.mcw.edu/doc/00719.html
|
|
|
