|
|
Toxoplasmosis
Submitted by Marion Brody, MD
Ring Enhancing Lesions in
Patients with AIDS
- Diagnoses to consider in anyone with multiple ring-enhancing lesions:
- Metastatic disease
- Demyelinating disease
- Infection
- Leading diagnoses in patients with advanced AIDS who have CNS abnormality:
- Toxoplasma encephalitis (T. Gondii)
- Primary CNS Lymphoma (EBV)
- PML (JC)
- HIV Encephalopathy (HIV)
- CMV Encephalitis (CMV)
- Other diagnoses to consider in patients with advanced AIDS who have CNS abnormality:
- TB (in developing countries)
- Staphylococcus, Streptococcus, Salmonella, Nocardia,, Rhodococcus, Listeria;
- Cryptococcus; Histoplasmosis; Candidiasis; Coccidioidomycosis; Aspergillosis; Trypanosomiasis; Herpetic meningoencephalitis; Neurocysticercosis; Meningovascular syphilis; Amebic abscesses
- How does the physician avoid a brain biopsy?
- Leading diagnoses in patients with advanced AIDS who have “Mass Lesions”:
- Toxoplasma encephalitis (T. Gondii)
- 50% of all brain lesions in AIDS patients.
- Primary CNS Lymphoma (EBV)
- 30% of all brain lesions in AIDS patients
- (PML, HIV-associated encephalopathy, and CMV encephalitis usually do not cause mass lesions)
- History
- Toxo
- Headache, confusion, +/- fever; focal weakness, seizures; if advanced, dull affect
- Lymphoma
- All of above and constitutional symptoms (night sweats, weight loss)
- PML
- Rapid neurologic decline (hemiplegia, visual field defects, ataxia, aphasia)
- HIV Encephalopathy
- Progressive memory loss, depression, movement disorders
- CMV encephalitis
- Confusion, focal deficits
- Laboratory tests
- Blood:
- Anti-toxoplasma IgG antibodies are almost always positive if patient has toxo encephalitis
- Toxo IgM Abs generally are not detectable in acute infxn; Toxo IgG quantitative levels do not reflect disease activity.
- Patients with toxo usually have CD4 < 100
- Patients with CMV encephalitis usually have CD4< 50
- A lumbar puncture is contraindicated if patient has lesions producing mass-effect and has focal signs
- CSF:
- Toxo, PCNSL, and PML shows <500 lymphs/uL, increased protein, normal glucose.
- Lymphoma may or may not show abnormal lymphocytes
- Toxo PCR is 50% sensitive, up to 100% specific.
- EBV PCR sensitivity/specificity varies with testing center
- JC virus PCR is up to 93% sensitive and specific
- CMV PCR is 80% sensitive, 90% specific
- Imaging on CT and MRI
- Toxoplasma Encephalitis
- Thin-walled ring-enhancing lesions, surrounding edema; rarely diffuse encephalitis
- Multiple lesions 80%
- Usually hyperintense with hypointense rim on T2 (can have decreased signal in central areas from calcium and hemorrhage)
- Basal Ganglia, G/W junction; parietal, frontal, thalamus
- More likely to appear in posterior fossa than PCNSL
- < 4 cm
- Primary CNS Lymphoma
- Ring-enhancing lesions, surrounding edema
- Multiple lesions 50%
- Variable signal on T2; isointense or hypointense on T1
- Basal Ganglia, deep white matter
- More likely to cross corpus callosum or occur in periependymal areas than TE
- Can be > 4cm
- PML:
- Multiple areas of demyelination, without contrast-enhancement or edema
- Bilateral, asymmetric; hypointense on T1, hyperintense on T2
- Can see atypical enhancing lesions with immune reconstitution syndrome
- Periventricular and subcortical white matter (rarely grey matter)
- HIV Encephalitis:
- Indistinct lesions in subcortical white matter
- Symmetric; hyperintense on T2
- CMV Encephalitis:
- Scattered micronodules in the cortex, BG, brain stem, and cerebellum; or
- Large ventricles with periventricular enhancement/hyperintensity on T2; or
- Ring-enhancing lesions with edema
- Other imaging modalities:
- SPECT – lymphoma greater thallium uptake than Toxo
- PET – lymphoma greater glucose + methionine uptake than Toxo
- Perfusion MRI – Increased flow in lymphoma, decreased in Toxo
- MR Spectroscopy – TBA
- Take home points
- 90% likelihood it’s Toxo if all of the following criteria are met:
- Toxo IgG (+) in serum.
- Patient with a CD4 < 100 is not receiving prophylaxis for Toxo
- Multiple ring enhancing lesions on CT or MRI
- In these cases, often patient is treated presumptively for Toxo
- If it’s Toxo, should see clinical improvement in 1 week (caveat: steroids can improve immediate symptoms by reducing brain edema without any true reduction in severity of infection)
- If it’s Toxo, should see radiographic improvement within 2 weeks
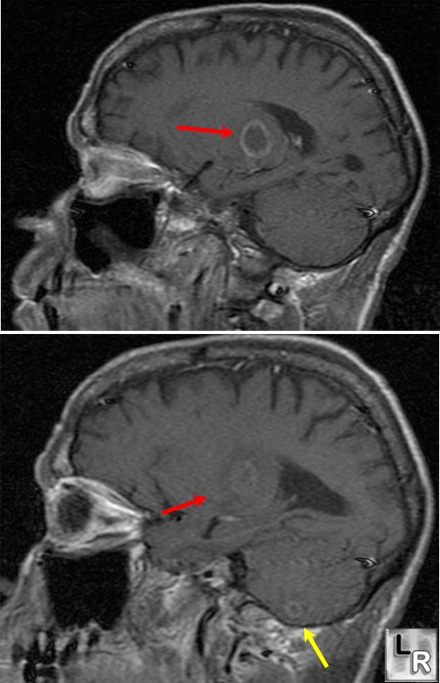
Toxoplasmosis. T1 weighted,
gadolinium-enhanced
sagittal MRI images of
the brain demonstrate
two
ring-enhancing lesions,
one (red arrows) in the
thalamus and the other
(yellow arrow)
in the cerebellum.
Chepuri, NB. Ring Enhancing Cerebral Lesions. In Magnetic Resonance Imaging of CNS Disease,
York DH (Ed.), 2002. Mosby, Philadelphia, PA.
Heller, HM. Toxoplasmosis in HIV-infected patients. In: Up To Date, April 23, 2005, Aronson, MD, Fletcher, RH, Fletcher, HW, Rind, DM (Eds.) Waltham, MA.
Koralnik,
IJ. Approach to HIV-infected patients with central
nervous system lesions. In: Up To Date, March 30, 2005, Aronson, MD, Fletcher, RH, Fletcher, HW, Rind, DM (Eds.) Waltham, MA.
|
|
|
