|
|
Leptomeningeal Cyst
Growing Fracture
- Sometimes called a “growing fracture”
- Age
- Incidence
- Rare - <1% of pediatric skull fractures
- Clinical findings
- Usually detected by parents who note a soft, cystic mass developing on skull of child
- Pathogenesis
- Skull fracture with dural tear leads to herniation of pia and arachnoid layers (leptomeninges) through the dural tear
- Cerebrospinal fluid pulsations lead to progressive erosion of skull around the fracture site
- Margins of the fracture will still be apparent months after injury and there will be greater diastasis of the fracture as time goes on than when first injured
- Imaging findings
- Angular, linear lytic lesion in the skull with scalloped margins
- Brain extrusion may occur shortly after the fracture in neonates and young infants leading to focal dilatation of the lateral ventricle near the growing fracture
- MRI
- Cyst isointense with CSF and communicating with subarachnoid space
- Area of encephalomalacia underlying fracture (frequent)
- Intracranial tissue extending between edges of bone
- Treatment
- Surgical repair of the dura and resection of the cyst
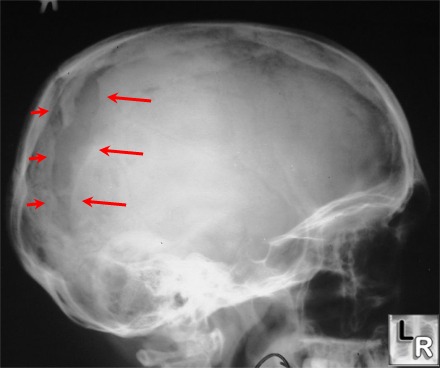
Left lateral radiograph
of the skull reveals a
sharply marginated, angular,
linear lucency
in the posterior
parietal-occipital region at
the site of a previous
linear skull fracture.
This is the characteristic
appearance of a
leptomeningeal cyst.
|
|
|
