|
|
Rheumatoid Arthritis
General Considerations
- Cause ─ unknown
- Possible genetic predisposition
- Questionable reaction to antigen from Epstein-Barr virus
- Age-Highest incidence 40-50 years
- Female preponderance 3:1 under the age of 40; equal distribution over 40 years
- Pathogenesis
- Injury to synovial endothelial cells leads to
- Synovitis with synovial hypertrophy which leads to
- Impaired nutrition with necrosis of cartilage and resultant
- Joint narrowing
Clinical findings
- Diagnostic criteria of American Rheumatism Association (at least 4 criteria should be present):
- Morning stiffness for >1 hour
- Swelling of >3 joints, particularly of wrist, metatarsophalangeal or proximal interphalangeal joints for >6 weeks
- Symmetric swelling
- Typical radiographic changes
- Rheumatoid nodules
- Biochemical tests
- Positive rheumatoid factor
- Rheumatoid factor
- Positive in 85-94%
- IgM-antibody
- Antinuclear antibodies
- LE cells
- Positive latex flocculation test
Imaging Findings
- Location
- Usually symmetric involvement of true, diarthrodial joints
- Target areas
- Proximal joints of hands and wrists
- All five MCP, PIP joints and interphalangeal joint of thumb
- All wrist compartments
- Especially radiocarpal, inferior radioulnar, pisiform-triquetral joints
- Early signs
- Fusiform periarticular soft-tissue swelling (result of effusion)
- Regional osteoporosis (disuse and local hyperthermia)
- Widened joint space (rare to see)
- Marginal and central bone erosions in small joints of hands and wrists
- Less common in large joints
- Site of first erosion is classically base of proximal phalanx of 4th finger
- Erosion of the ulnar styloid and narrowing of the distal radioulnar joint
- Atlantoaxial subluxation >2.5 mm (in >6%)
- Giant synovial cysts
- Late signs
- Diffuse loss of interosseous space
- Flexion and extension contractures with ulnar subluxation and dislocation
- Marked destruction of joint spaces
- Extensive destruction of bone ends
- Bony fusion
- Elevation of humeral heads (from rotator cuff tears)
- Resorption of distal clavicle
- Erosion of superior margins of posterior portions of ribs 3-5
- Destruction and narrowing of disk spaces
- Irregular vertebral body outlines
- Absence of osteophytosis
- Destruction of zygapophyseal joints without osteophyte formation
- Resorption of spinous processes
- "Stepladder appearance" of cervical spine due to subluxations
- Protrusio acetabuli (from osteoporosis)
- Synovial herniation and cysts (eg, popliteal cyst)
- Calcaneal plantar spur
Complications
- Extra-articular manifestations (76%)
- Felty’s syndrome (<1%)
- Rheumatoid arthritis (present for >10 years)
- Splenomegaly
- Neutropenia
- Age
- F > M
- Rare in African-Americans
- Sjögren’s syndrome (15%)
- Keratoconjunctivitis
- Xerostomia
- Rheumatoid arthritis
- Pulmonary manifestations
- Pleural effusion, mostly unilateral, without change for months
- Usually not associated with parenchymal disease
- Interstitial fibrosis with lower lobe predominance
- Rheumatoid nodules (30%)
- Well-circumscribed
- Peripheral
- Frequent cavitation
- Caplan’s syndrome
- Hyperimmune reactivity to silica inhalation with rapidly developing multiple pulmonary nodules
- Pulmonary hypertension secondary to arteritis
- Subcutaneous nodules
- In 5-35% with active arthritis over extensor surfaces of forearm
- Other pressure points (eg, olecranon) without calcifications (DDx to gout)
- Cardiovascular involvement
- Pericarditis (20-50%)
- Myocarditis (arrhythmia, heart block)
- Aortitis (5%) of ascending aorta ± aortic valve insufficiency
- Rheumatoid vasculitis
- Neurologic sequelae
- Distal neuropathy (related to vasculitis)
- Nerve entrapment (atlantoaxial subluxation, carpal tunnel syndrome, Baker cyst)
- Lymphadenopathy (up to 25%)

Rheumatoid Arthritis. Severe rheumatoid arthritis of the wrist and hand. The ulnar styloid is destroyed with the rest of the distal ulna (white arrow), there is destruction of the carpal bones (yellow arrow) and there is dislocation of the 1st metacarpal on the destroyed trapezium (blue arrow). All of the bones are osteopenic.

Rheumatoid Arthritis, both feet. There are innumerable intra-articular erosions (white circles) involving not only the great toes but all toes. There are multiple subluxations of the joints (white arrows)
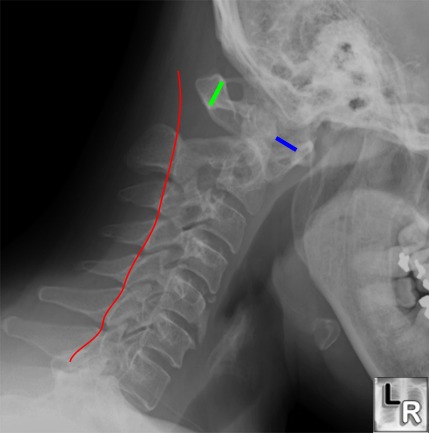
Lateral
radiograph of
the neck with
the head in
flexion shows
an increased
distance
between
the anterior
border of the
dens and the
posterior
border of the
anterior
tubercle of C1
(blue line)
from
ligamentous
laxity caused
by rheumatoid
arthritis. The
"pre-dentate
space," as
this is
called, should
be less than 3
mm in the
adult. The
red line
above should
smoothly
connect all of
the
spinolaminar
white lines of
each vertebral
body but
clearly is
directed
posterior to
the
spinolaminar
white line of
C1 (green
arrow) since
C1 is subluxed
forward on C2.
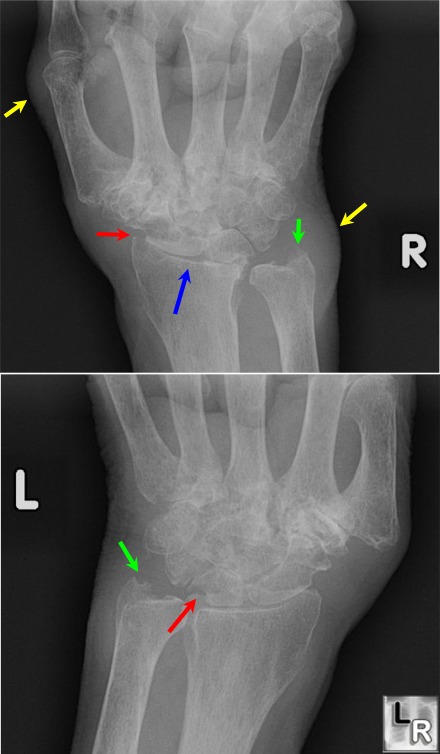
Frontal images of both the right(above) and left wrists (below) show advanced changes of rheumatoid arthritis with soft tissue swelling (yellow arrows), narrowing of the radiocarpal joint space blue arrow). erosions (red arrows),
and destruction of the ulnar styloid (green arrow). The intercarpal joints are destroyed as are all of the carpal-metacarpal joints of both hands. Note the symmetric appearance of the disease.
For more information, click on the link if you see this icon 
|
|
|
