|
|
The Lateral Neck
Croup
- Soft tissue measurements on the lateral neck image
- At C3: <3 mm (less than 1/3 AP diameter)
- At C6: < the AP width of C6 vertebral body
- Retropharyngeal Space
- Contains lymphatics that drain
- Nasopharynx
- Adenoids
- Posterior nasal sinuses
- These chains atrophy after age 4
- Retropharyngeal abscess
- Almost all occur before age 6
- 50% between 6-12 months
- Most common pathogens are
- Staph aureus
- Group A Beta hemolytic Strep
- Hemophilus
- Clinically
- Prodromal nasopharyngitis
- Severe throat pain with drooling
- Dysphagia
- Hyperextension of the head
- “Hot potato” muffled voice
- In adults, usually 2° trauma to oropharynx
- Retropharyngeal perforation
- Causes
- Trauma to esophagus or trachea
- Penetrating injuries from weapons
- Perforation from within
- Chicken bone
- Mediastinal emphysema tracking into neck
- Retropharyngeal abscess 2° gas-forming organism
- Imaging findings of retropharyngeal perforation
- Streaks of air in soft tissues of neck
- Anterior displacement of pharynx
- Associated pneumothorax possible
- Cervical or mediastinal air seen in 60% of cases of ruptured esophagus
- Upper airway infections-The Big Two
- Croup
- Laryngeotracheobronchitis
- Usually viral
- May be difficult to distinguish from early retropharyngeal abscess
- Occurs at age 6 months to 2 years
- Younger than epiglottitis
- The three major findings of croup
- Distension of the hypopharynx
- Distension of the laryngeal ventricle
- Haziness or narrowing of subglottic space
- Epiglottitis
- Most commonly H. flu type B
- Peak incidence now closer to 6-7 years
- Croup occurs from 6 months to 2 years
- Lateral radiograph -- erect position only
- Supine position may close off airway
- Imaging findings
- Epiglottis is enlarged
- Appears thumb-like
- Aryepiglottic folds are thickened
- Pre-epiglottic space (vallecula) is smaller than normal
- In many cases, it’s obliterated
- Impacted esophageal foreign bodies
- Food or true foreign bodies
- Chicken bones (opaque), fish bones (non-opaque)
- Coins, toy trucks
- Most often they impact just below cricopharyngeous (70%)
- Another 20% impact at the level of the aortic arch
- Another 10% at EG junction
- Once past the esophagus, most foreign bodies will pass through the GI tract
- Clinical findings of an impacted esophageal foreign body
- Dysphagia and odynophagia most commonly
- Even if FB passes, many complain of pain referable to cervical esophagus
- Always check for lead lines in children
- Chicken bones are usually opaque
- Fish bones contain less calcium and usually are not
- Plain films usually do not demonstrate the FB but are still obtained first
- If negative, then either contrast esophagram or CT if high index of suspicion
- Treatment
- Removal is most often performed using endoscopy
- Temporization and surgery are other options
- An ingested button battery lodged in esophagus must be removed immediately
- Complications of an impacted foreign body
- Perforation
- Longer the FB remains impacted (>24hrs), higher incidence of perforation
- Stricture
- Diverticulum formation

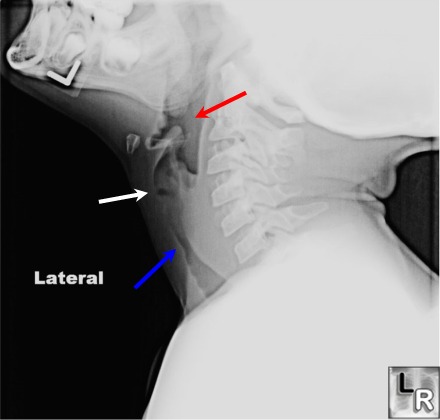
Croup. Soft tissue lateral neck demonstrates a dilated hypopharynx (red arrow),
dilatation of the laryngeal ventricle (white arrow) and narrowing of the
subglottic trachea (blue arrow).
For this same photo without arrows, click here
Croup. Soft tissue lateral neck (edge enhanced)
shows a slightly dilated hypopharynx (red
arrow),
dilatation of the laryngeal ventricle (white
arrow) and narrowing of the subglottic
trachea (blue arrow)
For more information, click on the link if you see this icon 
|
|
|

{kind=link}